

The RIPCHD.OR project is a deep and rigorous dive into a single space within an increasingly prevalent health care setting.
Image courtesy of Clemson University
Great strides have been made in building the knowledge base in health facility design. As a result, health care environments are clearly better, safer, and more efficient and effective than those of the 20th century.
Yet, as a scientific discipline, the evidence-based design (EBD) field is still in its infancy. There remains a need for replication of earlier studies to help validate original findings, or challenge them.
It is therefore important that design professionals are modest in their claims and rigorous in the translation and application of research into design practice. To do otherwise risks being proven wrong after buildings are built, and, more importantly, it risks compromising the credibility of research in the discipline.
Scientific research is inherently about seeking answers to specific questions and controlling variables, yet health care settings are complex. It is difficult to isolate cause and effect. The design of health care settings must inevitably address multiple drivers and variables that are often in conflict. Each project is unique with a distinct context, set of variables and conditions. Rigorous research is also slow and methodical by nature as research moves from proposal to funding through institutional review board to data collection, compilation and translation of finding, and finally into dissemination and peer review. Yet design moves relatively rapidly. So, the challenge is to provide rigorous, useful, timely and applicable knowledge that can be applied broadly and translated into useful forms that can effectively and responsibly guide design decision making and action.
Two recent initiatives at Clemson University attempt to provide useful and applicable information to inform designers and design decision making:
- The American Institute of Architects/Academy of Architecture for Health (AIA/AAH) case study initiative was created to capture and consistently document best practices in health care design through its design awards program. While not a research process per se, it provides information in a systematic format that could be used for research while serving as a benchmarking resource immediately.
- The Realizing Improved Patient Care through Human Centered Design in the Operating Room (RIPCHD.OR) project is a deep interdisciplinary research study into a single clinical space, the ambulatory surgery OR.
A closer look at these two design research projects follows.
Case study research
Clemson’s Graduate Program in Architecture + Health has historically utilized case study research in its studio projects. Over time, it honed this process into a standardized graphic format. The AIA/AAH Research Initiatives Committee established an AIA/AAH case study library by utilizing Clemson’s format to document peer-reviewed benchmarks from AIA/AAH Healthcare Design Awards projects. The case study library officially rolled out in late 2016, with a goal of bridging the gap between research and practice.
The initial purposes of this effort was to identify peer-reviewed case studies to share with the health care sector, use the AIA/AAH Health Care Design Awards program as a source for case studies, define a standardized format and encourage firms and their clients to use it, and create an AIA/AAH case study repository or library for sharing case studies.
The goal is to establish a more focused and formal approach to sharing of design award-winning project information by creating a database for a qualitative and comparative baseline for developing scalable metrics that, in turn, will enable best practice benchmarking analyses on past projects, which may eventually lead to more rigorous research opportunities (e.g., post-occupancy evaluations).
Since the launch of the AIA/AAH case study library in 2016, this effort has added projects from the 2013, 2014, 2015 and 2016 AIA/AAH Healthcare Design Awards. It now totals 30 case studies. Work is also underway on the 2017 and 2018 projects, which will add another 14 projects to the library.
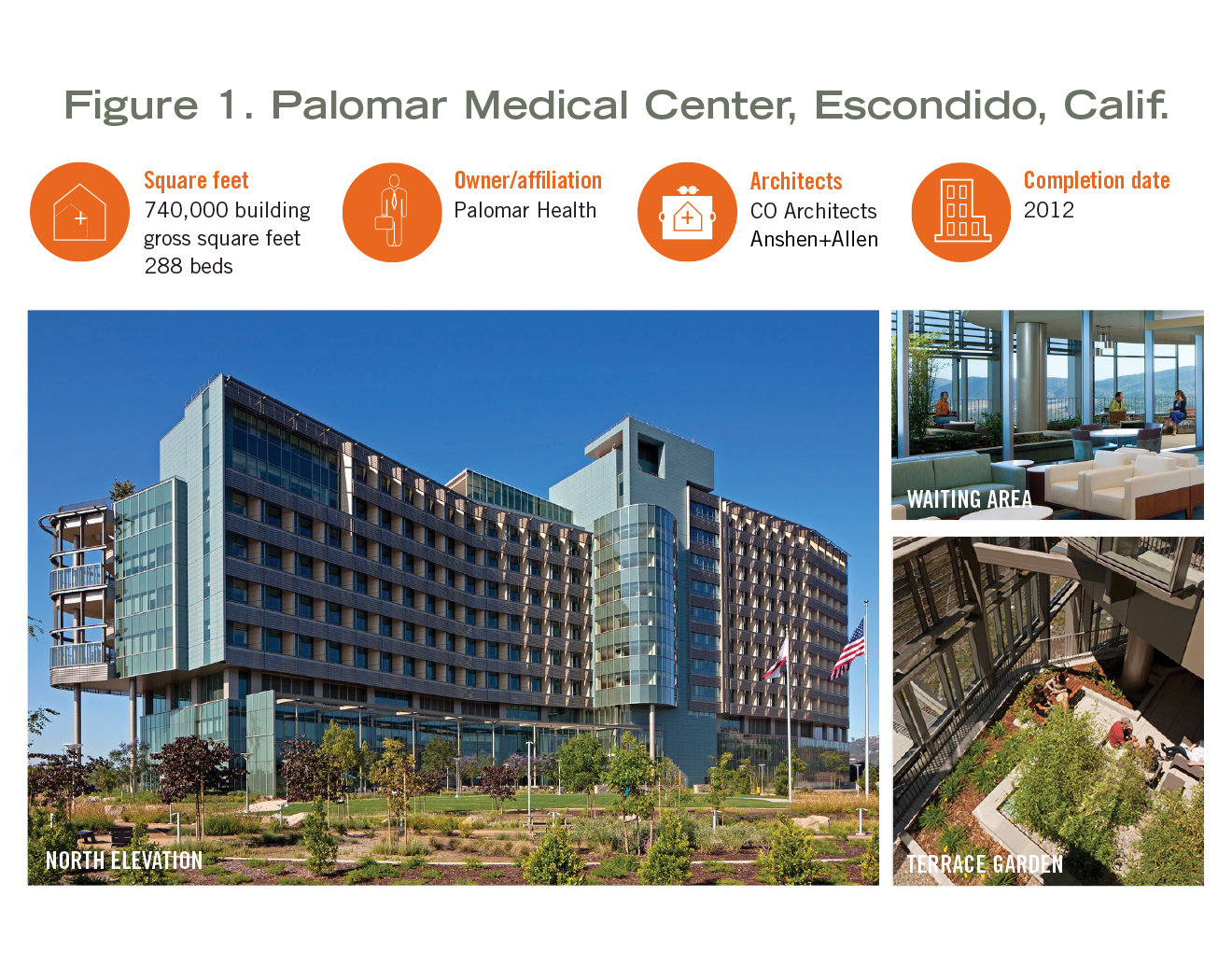
In addition to adding case studies every year, the committee took a deeper dive in 2018 into “benchmarking” acute care nursing units and patient rooms for Palomar Medical Center (see Figure 1) and Rush University Medical Center.
The intent is to produce a subset within the library of nursing unit and patient room typologies for more detailed departmental and key clinical space comparison and benchmarking.
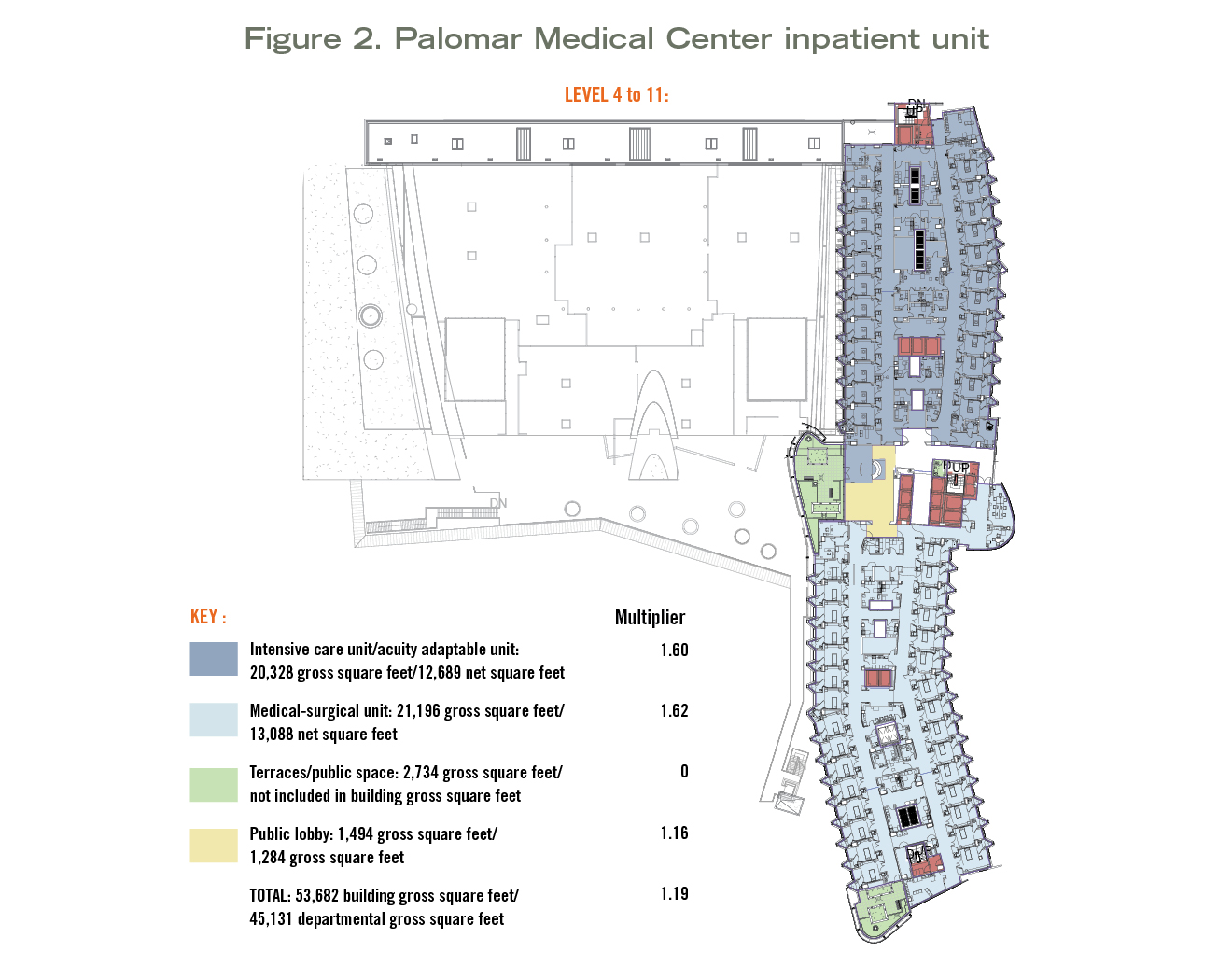
The typical case study highlights key design intentions of each project and shows photographic images to help identify design features that address those intentions. The format also identifies the project team, overall building gross square footage and completion date, as well as floor-by-floor interdepartmental net to gross square footages and net to gross factors. It also identifies minimum and maximum travel distances for patient and staff travel within key departments. Typical and average net square footages are identified for key clinical spaces (see Figure 2). Finally, award jury comments are also added to help explain the award-winning features.
As part of this deeper dive into benchmarking, a detailed departmental takeoff for a typical floor plan for the medical-surgical floors and the critical care floors was conducted on both hospitals, utilizing the takeoff procedure described by David Allison, AIA, ACHA, and D. Kirk Hamilton, FAIA, FACHA, in the January 2008 final report on “Analysis of Departmental Area in Contemporary Hospitals: Calculation Methodologies & Design Factors in Major Care Departments.” The AIA/AAH and now the American Society for Health Care Engineering are encouraging this as the health care sector standard for building square footage takeoffs.
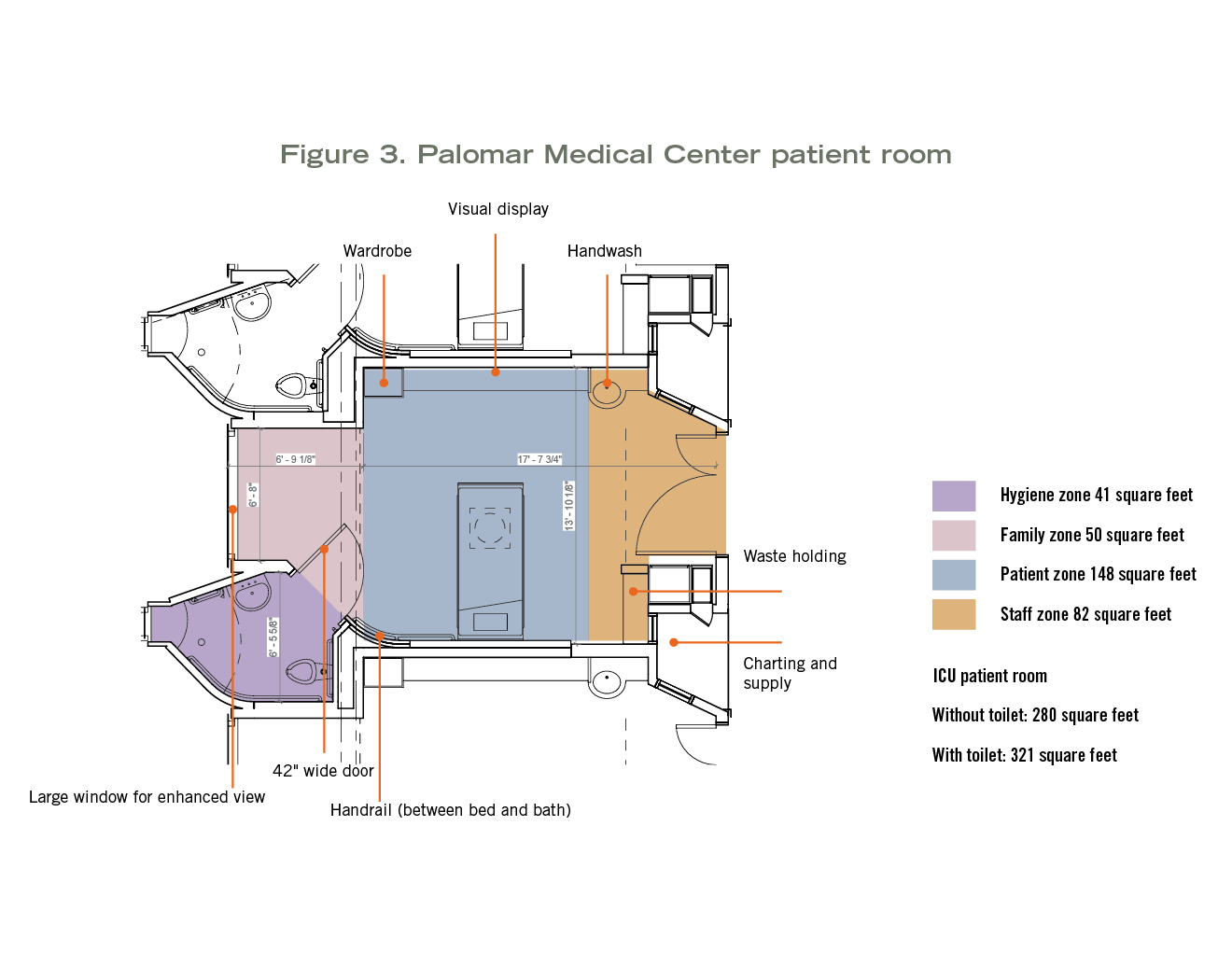
Detailed patient room takeoffs were also included in these more detailed case studies with key design features noted (see Figure 3). The plan is to perform additional inpatient unit and departmental takeoffs on other case study projects over time as well as to add additional detailed inpatient (and outpatient) departmental takeoffs from other case studies within the library.
Examining a series of health care facilities in a consistent format is a critical step for creating a database repository; and identifying and then validating “best practices” and “rules of thumb” comparisons are a prerequisite for performance-based design. The AIA/AAH hopes that the case study library will become more robust over time and help health care planning and design professionals as well as researchers to utilize benchmarking for research-informed and performance-based design, and enable further research such as post-occupancy evaluations and comparative studies.
OR prototyping project
RIPCHD.OR is a four-year patient safety learning lab (PSLL) project funded by the Agency for Healthcare Research and Quality. It involves a multidisciplinary, human-centered approach to study the ambulatory surgery OR to improve safety, ergonomics and operational efficiency.
It includes a collaboration between faculty and students in the Graduate Program in Architecture + Health,
and industrial engineering and management through the Center for Health Facilities Design and Testing at Clemson University, along with clinicians and research faculty at the Medical University of South Carolina (MUSC) in Charleston.
Project process. The overall project involves three teams focused on different aspects and scalar areas of inquiry of the OR milieu. Project one involves the focused study of the anesthesia workspace. Project two involves the study of door openings and traffic flow into and out of the OR. Project three examines the integrated OR space along with immediately adjoining and connected support spaces and zones.
RIPCHD.OR was conceived as an iterative research, design, test, refine and retest process where a design prototype was designed, built as a mockup and evaluated at increasingly higher levels of fidelity through iterations of the prototype in both virtual and physical simulations.
Year one involved an extensive literature review and best practice case study analysis, Facility Guidelines Institute code analysis, video observation, and detailed coding and analysis of a cross section of pediatric and orthopedic ambulatory surgery procedures in existing ORs at MUSC.
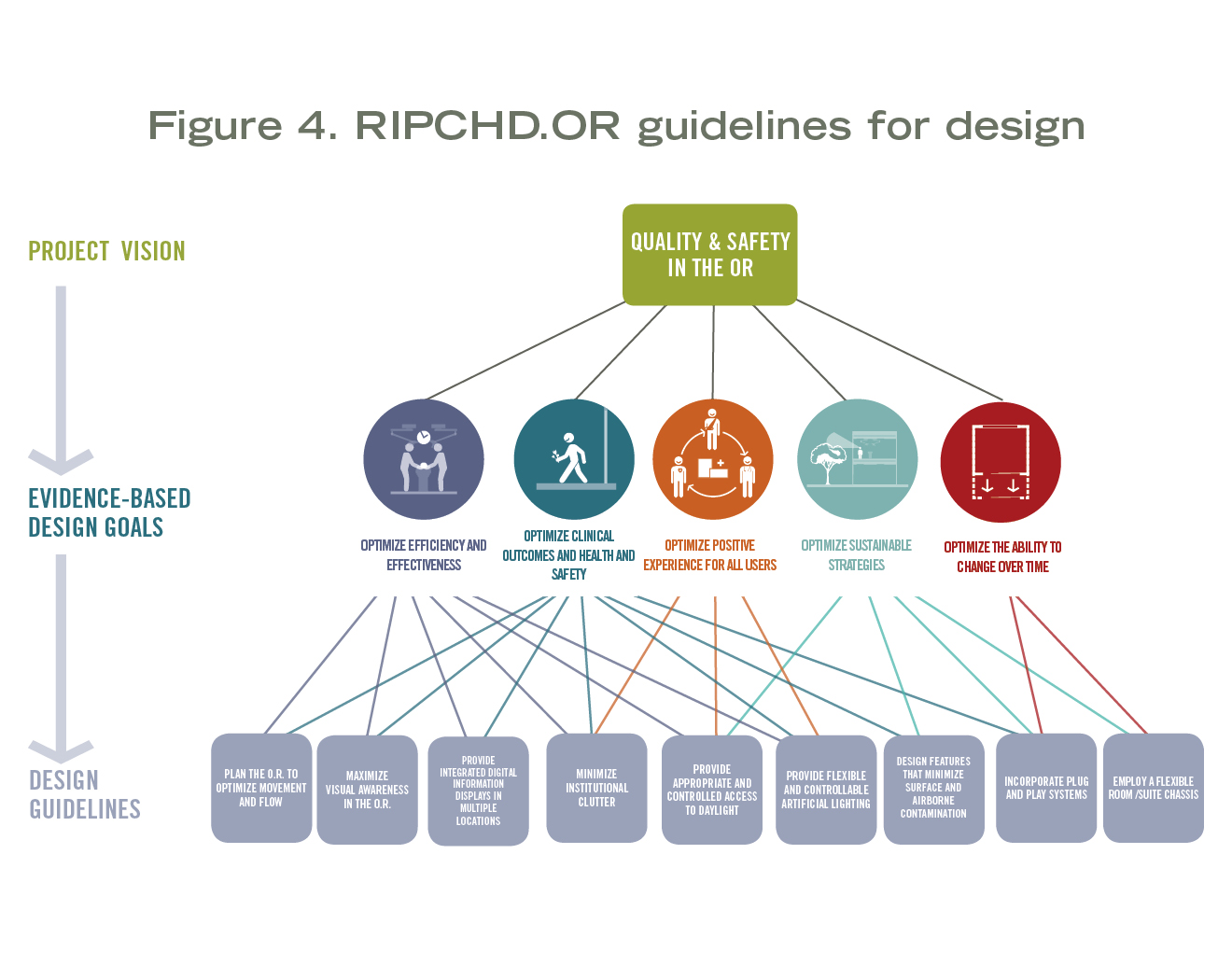
The research collected in year one was then used to inform a visioning workshop to identify critical issues in design and process, define the project vision, establish EBD design goals and frame a series of design guidelines (see Figure 4). The workshop involved students and faculty, clinicians, the multidisciplinary research team, an advisory board and industry partners.
The workshop kicked off the design of a prototype executed by Master of Architecture + Health students in collaboration with the research and clinical team at Clemson and MUSC in year two. Initial design ideas were developed as conceptual design drawings and a large physical model along with a tape on the floor mockup at Clemson’s Charleston Design Center near MUSC.
The tape on the floor mockup helped evaluate, determine and confirm the basic footprint or chassis of the OR and identify initial options for door and window locations, placement of the OR table, and other critical movable equipment and supply storage along with zoning of the room.
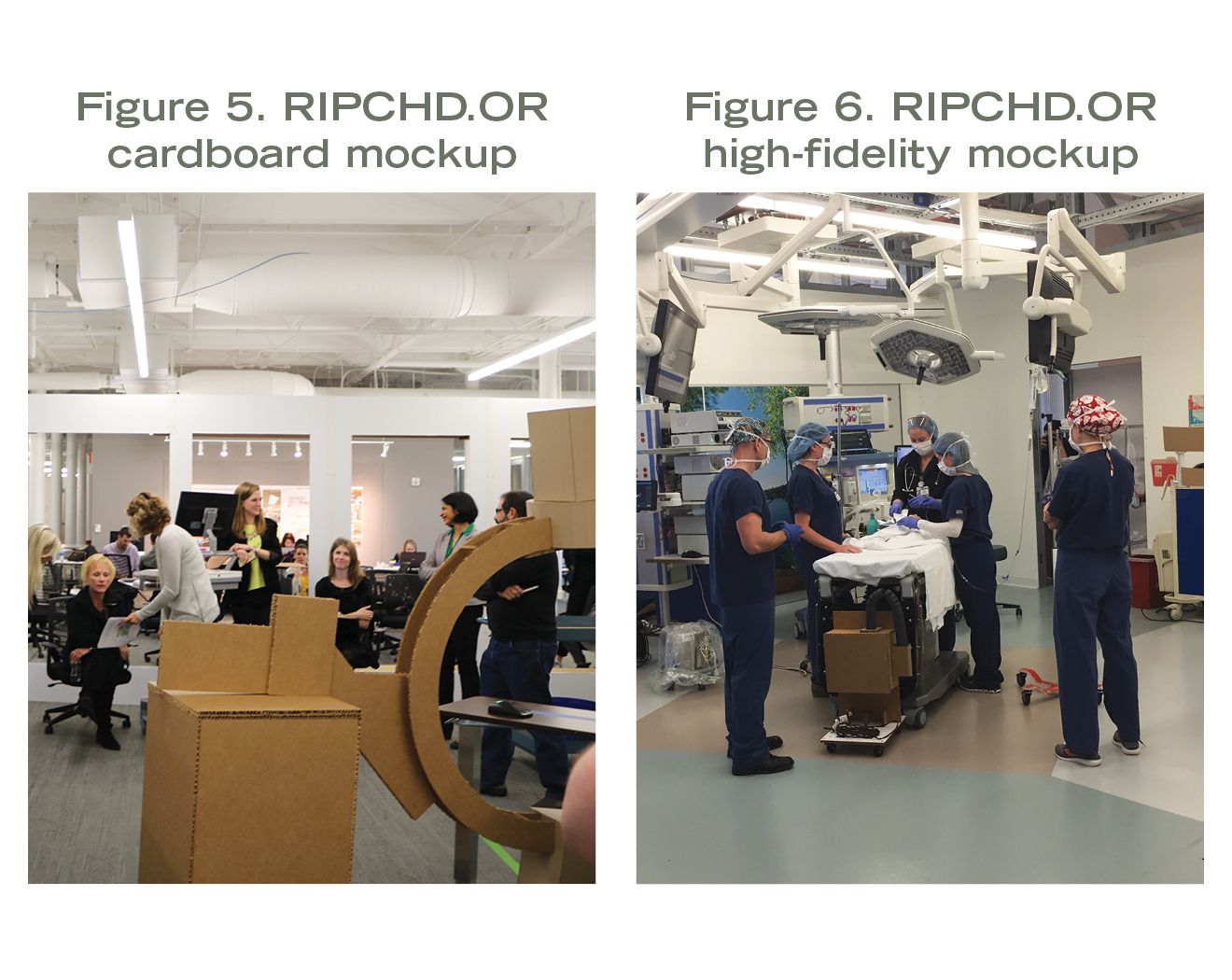
This led to design refinements and the construction of a plug-and-play cardboard mockup that allowed further simulation testing of equipment and supply placement, movement patterns for staff-patient-equipment entry and exit, along with confirmation of OR table location and orientation and five discrete work zones in the OR (see Figure 5).
The results of these structured simulations led to further design refinement and construction of a high-fidelity prototype involving metal stud walls, wall panels, sliding doors, overhead booms and lights along with boom and wall mounted video display equipment (see Figure 6). Additional movable equipment was brought in to fully outfit the OR for more complete surgical procedure simulation during preoperative, intraoperative and post-operative phases of several pediatric and orthopedic procedures using a computerized human simulator and simulation training protocols.
A virtual model of the OR space was also tested by translating the mapping of movement during observed surgical procedures in year one into new versions of the OR space with several configuration and dimensional variations.
Years three and four involved further simulation testing, compilation of findings, continued publication and presentation of both the process and results of the study. MUSC also designed and built the first of two ASCs informed directly by the study. A web-based OR design tool and checklist was also developed and can be accessed at http://ordesign.clemson.edu/or_design_toolkit. This resource is intended to enable design professionals to work in collaboration with clinicians and other constituencies to develop and evaluate EBD-based solutions for OR design.
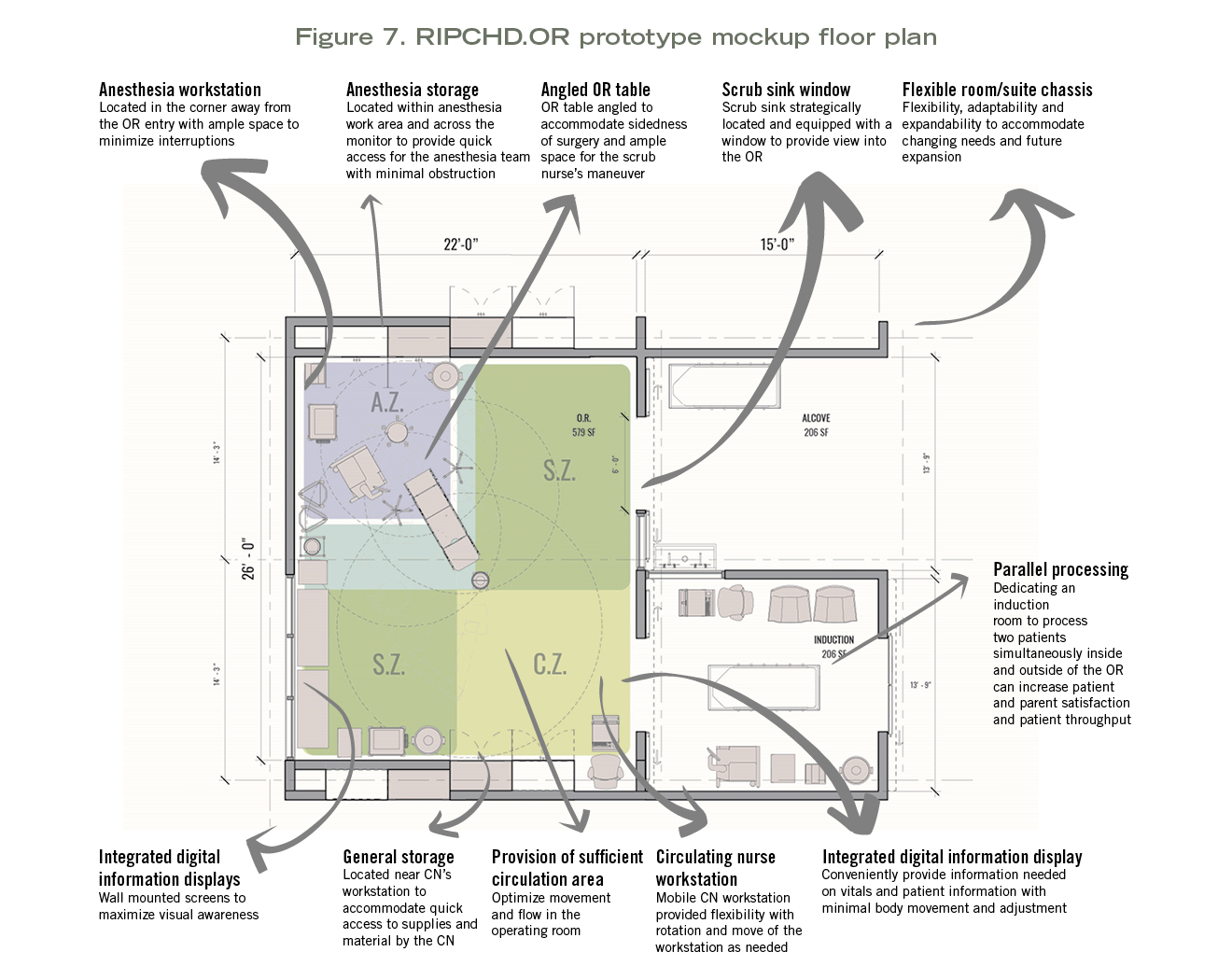
Design findings. From a physical design standpoint, the RIPCHD.OR research-design-research project identified several design features that indicated potential improvements in OR design (see Figure 7).
The unique position of the OR table — off-centered and diagonal in the room — allowed improved movement for the circulating nurse while minimizing task disruptions, conflicts with others in the room and moveable equipment. It also enabled efficient movement into the OR and transfer of the patient to/from the OR table.
Finally, it situated the anesthesia workspace in a protected and effectively organized work zone diagonally opposite the entry and primary circulation zone in the room. This also enabled better utilization of the dead space that often exists in the back corner of the room behind the anesthesia boom and machine and the sterile work area at the patient’s right side for common mid-body procedures.
This position also enables the table to be rotated for procedures where the surgeon is positioned at the patient’s head while maintaining effective positioning of the anesthesia team and equipment.
Five distinct work zones can be maintained with minimal conflicts, including the patient (OR table) zone, a sterile work zone on either side of the patient, a protected anesthesia work zone and a circulation zone. Another feature of the room involved employing a mobile circulating nursing workstation that can be parked in an alcove when not in use and then positioned to give a clear line of sight to the patient and procedure during the perioperative phase irrespective of the positioning of the OR table and surgical team.
Two ancillary spaces were identified in the simulations as having the potential to enable parallel processing and improve throughput and transition between procedures. For short pediatric procedures, an induction room was introduced and tested. Given induction typically takes longer than the procedure itself, this allowed one patient to begin induction while another was still in the OR.
Since induction can be stressful for pediatric patients, the induction room model is also a more patient- and family-centered model that allows parents to be present during induction while not compromising the OR itself. The study team observed the induction room model in operation at the Children’s Seattle Bellevue ASC during case study research, and the clinician teams at MUSC embraced it after simulation testing in the prototype. Orthopedic procedure simulation testing suggested that a post-operative instrument breakdown room could lead to improved throughput and process improvement by shortening the turnaround time in the OR itself.
The RIPCHD.OR prototype was ultimately conceived as a flexible chassis with a size, shape and layout designed to accommodate a variety of procedures, associated equipment, and detailed room configurations and appointments.
The core chassis involved the 22-foot by 26-foot room with a 2-foot deep boundary zone for doors, windows, scrub sinks, recessed storage and equipment alcoves both within and outside the room. Secondary and tertiary zones along both the short and long side of the room are envisioned to accommodate a variety of immediately adjacent support spaces, including induction, instrument breakdown, procedure control, equipment and storage rooms, and entry.
Depth and breadth
These two initiatives represent knowledge gathering and generation with distinct levels of depth and breadth.
The case study library is intended to gather information systematically and consistently on projects that have been deemed through a design peer review process to be noteworthy. This information can be used immediately to share more accurate information on these projects beyond what is typically found in publications and marketing materials. The consistent documentation of these projects can also ultimately be used to conduct future research on individual projects to evaluate their performance as well as conduct comparative studies across individual projects.
Conversely, the RIPCHD.OR project is a rigorous dive into a single space within an increasingly prevalent care setting. It represents a federal research grant over four years with significant funding and a large multidisciplinary team and process. It involved an iterative research-design-research process that addressed specific research questions and more general design hypotheses. It includes the translation of research knowledge into formats applicable to design and useful in the design decision-making process.
These initiatives cover a range of EBD practices and processes with varying levels of rigor, depth and breadth. It is hoped that both will lead to building the knowledge and evidence base in health care design and lead to more informed design and design decision making.
David Allison, FAIA, FACHA, is an alumni distinguished professor and director of Graduate Studies in Architecture + Health at Clemson University; Byron Edwards, AIA, ACHA, EDAC, is a professor of practice in Graduate Studies in Architecture + Health at Clemson University, and chair of the Research Initiatives Committee of the AIA/AAH; and Anjali Joseph, Ph.D., EDAC, is an endowed professor in architecture and health design and director of The Center for Health Facilities Design and Testing at Clemson University. They can be reached at adavid@clemson.edu, byrone@clemson.edu and anjalij@clemson.edu.
About this article: This feature is one of a series of articles published by Health Facilities Management in partnership with the American College of Healthcare Architects.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}