
Maybe the more pervasive, instantaneous media coverage of shootings and other violence in and around the nation's hospitals has raised awareness of security threats. Or, perhaps, it's the more brazen acts of aggression against physicians, nurses and other staff by patients and family members that recently has caught the nation's attention.
 |
| Click above image to download a full PDF. |
Whatever the case, hospital security is being assessed with greater concern and in more detail than ever before. The general assumption tends to be that violence in hospitals is on the rise. But is it? And, if so, how are hospitals responding to this trend?
Over the past year, 23 percent of hospitals reported an overall increase in attacks and assaults, compared with 10 percent reporting a decrease; 34 percent reported a rise in patient and family violence against emergency department staff versus 7 percent reporting a drop; and 29 percent reported an uptick in patient and family violence against other staff, compared with 7 percent reporting a decline.
These are some of the key findings from the 2011 Hospital Security Survey conducted in June by Perception Solutions for Health Facilities Management (HFM) and the American Society for Healthcare Engineering (ASHE). The survey was sponsored by Boca Raton, Fla.-based ADT Security Services Inc.'s Healthcare Solutions group.
 Nearly 600 hospital officials in charge of security — 16 percent of those invited to participate — responded to the nationwide survey. Fifty five percent of respondents were facility vice presidents or directors, 29 percent were security or safety directors and 16 percent had other titles.
Nearly 600 hospital officials in charge of security — 16 percent of those invited to participate — responded to the nationwide survey. Fifty five percent of respondents were facility vice presidents or directors, 29 percent were security or safety directors and 16 percent had other titles.
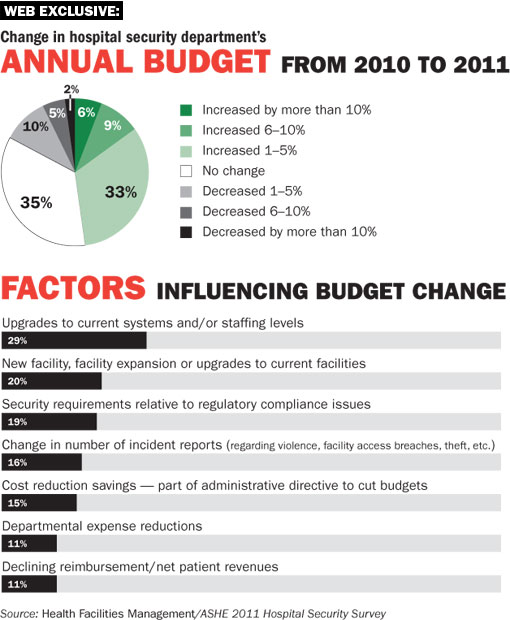
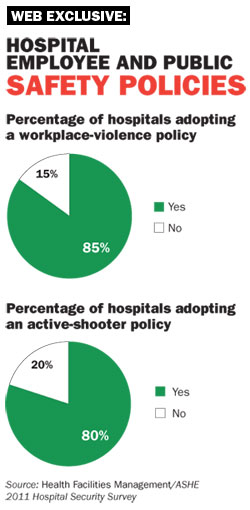
Despite the tough financial environment facing hospitals, nearly half the respondents said their security department's budget increased in 2011, while more than a third said there was no change. Almost 70 percent said their hospital's security strategic plan had been updated within the past 12 months. In addition, a large majority said their facilities had adopted workplace-violence and active-shooter policies to prepare staff for handling emergencies.
The most common systems being implemented by hospitals are electronic access control, digital video surveillance and vendor management systems. The most common systems hospitals plan to implement over the next two years include radio-frequency identification (RFID) systems for tracking equipment, supplies, patients and staff; and mass notification systems for emergency preparedness.
Beefing up systems
"I'm not surprised by the rise in assaults, because people are very stressed as a result of the state of the economy," says Skip Smith, CHFM, SASHE, vice president of supply chain, clinical engineering, and facilities management for Catholic Health Initiatives and president of ASHE. "But I see that people are doing a better job of risk-assessing their security issues."
"It's a different society out there than we've seen, and security has to be there so our clinicians and employees have the ability to provide care in a safe and secure environment," agrees Kevin Weeks, director of marketing at ADT Healthcare Solutions. "I'm encouraged that close to 70 percent of the hospitals are increasing their security budgets or keeping them level. That's positive."
"Our budget for technology and security staff that support our emergency and inpatient mental health areas increased significantly last year," adds Tom Smith, director of hospital police and transportation at University of North Carolina (UNC) Hospitals, who participated in the survey. "It helps a lot to receive support from clinical leadership as they respond to safety concerns expressed by staff."
The heightened focus on security comes as hospitals have experienced several violent incidents and threats in recent years. High-profile cases last year included the shooting of a physician at Johns Hopkins Hospital by a patient's son, who then killed his mother and himself, and the strangulation murder of a psych tech by a patient-inmate at Napa State Hospital in California.
Violence by the numbers
Government statistics tell a disturbing story. Each year there are an estimated 2,600 nonfatal assaults on hospital staff — a figure many believe would be much higher if hospital staff reported all assaults — according to "Violence: Occupational Hazards in Hospitals," a 2002 study by the National Institute for Occupational Safety and Health (www.cdc.gov/niosh/docs/2002-101/). Using 1999 Bureau of Labor Statistics (BLS) data, NIOSH said the rate of assaults against health care workers was 8 per 10,000, compared with 2 per 10,000 for workers in all private-sector industries.
More recently, a BLS report examining workplace safety from 2003 to 2007 found that nearly 60 percent of all nonfatal assaults and violent acts in U.S. workplace settings occurred in the health care and social assistance industry (www.bls.gov/opub/cwc/sh20100825ar01p1.htm). Additionally, while homicides and shootings in health care settings are rare, there were 73 murders in health care settings, including 20 in hospitals from 1997 through 2009, according to government figures (www.bls.gov/iif/oshwc/cfoi/work_hom.pdf).
Nursing staff in emergency departments (ED), intensive care units and psychiatric units are at a particularly high risk of being victims of violence. More than 1 in 10 ED nurses surveyed last year said they had been attacked in the previous week, according to the Emergency Nurses Association (www.ena.org/IENR/Documents/ENAEDVSReportAugust2010.pdf).
Many observers attribute the perceived increase in violence in hospitals to heightened stress faced by patients, family members and staff as increasing numbers of unemployed, uninsured, drug-using and mentally ill people seek care they can't access elsewhere.
"There's a mental health crisis in this country," says UNC's Smith. "There are far fewer community resources for mental health care, so these patients are showing up in the ER much sicker and more prone to violence, and they stay longer once they get here. We're all trying to find ways to manage them in a safe, humane way."
"Mental health patients and drug users account for a piece of it," Weeks comments. "But people with no previous criminal or mental health background also are acting out because of unemployment, lack of insurance, waits in the ED, and concern about their relatives in the hospital."
Push for programs
Due to the increased attention to violence, the Joint Commission, hospital industry groups, federal and state regulators, and hospital employee unions have pressed for better security programs and more complete reporting of incidents.
The International Association for Healthcare Security and Safety (IAHSS), for instance, is releasing comprehensive new guidelines this fall for optimizing security in the construction and renovation of health care facilities.
"Up until recently, architects would come in and do their thing, and security was an afterthought," says Bryan Warren, director of corporate security for the Carolinas HealthCare System, and president-elect of IAHSS. "In this day and age, we have to reverse that trend."
One of the most controversial security issues is whether to have hospital security officers carry electronic control devices such as Tasers. The HFM/ASHE survey found that only 12 percent of survey respondents said their officers carry such devices, 9 percent said their hospitals are testing them, and 79 percent said they have no plans to use them. Hospital security directors interviewed for this article had mixed reactions to those findings.
"I'd like to see the number of hospitals using Tasers expand, because the Taser is a nonlethal device for controlling violent behaviors that are erupting in hospitals across the nation," says Scott Martin, director of security and parking at University of California–Irvine Healthcare, which has a Taser program. He notes that if security officers are properly trained, merely displaying the device stops the disruptive behavior in the large majority of cases.
 In contrast, Dave Jacques, vice president of support operations at Chesapeake (Va.) General Hospital, where security officers also carry Tasers, says he's not convinced these devices make the hospital safer. "It requires a lot of training and review, and you can't use a Taser just to subdue a patient unless you're going to charge the patient with a crime," he says. "But it's hard to [end a Taser program] because the staff perceives it to be safer for them."
In contrast, Dave Jacques, vice president of support operations at Chesapeake (Va.) General Hospital, where security officers also carry Tasers, says he's not convinced these devices make the hospital safer. "It requires a lot of training and review, and you can't use a Taser just to subdue a patient unless you're going to charge the patient with a crime," he says. "But it's hard to [end a Taser program] because the staff perceives it to be safer for them."
There's also no rush to equip hospital security officers with guns. Just 22 percent of survey respondents said their security officers carry a firearm or their hospital system is evaluating the use of firearms; 78 percent said they had no plans to use firearms.
Detecting danger
A related issue is the use of metal detectors to screen for guns and other weapons. Weeks says guns in hospitals are a growing concern, partly because of the spread of concealed carry laws.
But hospitals aren't moving to adopt metal detector systems. The survey found that only 13 percent of respondents said their hospitals had implemented them, while 7 percent are planning to do so in the next 24 months. Eighty percent had no plans to adopt them.
"I envisioned more hospitals would be installing metal detectors," Weeks comments. "But they won't provide deterrence if someone is not standing there to take the gun or knife away. The ability to staff this technology is an issue as well."
That theory gets support from John Hawksworth, chief of police at the Altoona (Pa.) Regional Health System, which has its own private police department with full police powers. He says his hospital is considering installing metal detectors at the ED entrance because it's getting more violent patients. "But the administrator still isn't sold on that yet because it would require putting an officer at the door 24/7," he says.
High-tech help
One piece of good news in the survey is that infant abductions in hospitals are down. More than a quarter of respondents said actual and attempted abductions have decreased, compared with only about 1 percent who said abductions have increased.
That decrease could be related to the survey's finding of growing use of various high-tech security measures, including electronic access control (91 percent); Internet-connected video surveillance (74 percent); mass notification systems for emergencies (65 percent, with another 21 percent planning to implement this in the next 24 months); integrated security, including video access control, biometric and card access readers (63 percent); and visitor management systems (41 percent, with another 25 percent planning to implement this in the next 24 months).
"I would think the growth of more stable and robust wireless technologies contributed to the drop in infant abductions," says Shane Meenan, director of healthcare sales for ADT-Advanced Integration.
RFID tracking technology in security is also growing. Meenan says these systems are particularly useful for preventing theft of equipment and supplies, and also help with regulatory compliance and resource allocation. Nineteen percent of respondents said their hospital had implemented RFID for tracking equipment, 13 percent for tracking supplies, and 13 percent for tracking patients, staff and vendors. Moreover, 24 percent, 19 percent and 16 percent, respectively, said they plan to implement such systems to track patients, staff and vendors in the next 24 months.
One important use of RFID is for patients who have impaired decision-making capacity and are at risk for elopement. Many facilities assign staff to sit with such patients. "The thinking is that RFID tags, combined with access control and video surveillance, will reduce the need for someone sitting one-on-one with the patient," UNC's Smith says.
Finally, given the potential for violence, hospital security officials increasingly are preparing for the worst. Four out of five respondents said their hospitals have adopted active-shooter policies, readying staff to deal with gun situations and working with local police to plan and practice emergency responses. Chesapeake's Jacques says his hospital will conduct its first active-shooter drill this fall.
Training is key
Despite hospitals' growing interest in beefing up their security hardware, some security professionals urge health facility professionals to focus on training staff how to assess and de-escalate potentially violent situations.
"The best camera in the world can't reach out and stop a bad guy from hitting you," Warren says. "We need more training for security and professional staff in how to handle these violent people, more than we need cameras to record the event."
Harris Meyer is a freelance writer based in Yakima, Wash., and Suzanna Hoppszallern is senior editor of data and research for Health Facilities Management's sister publication, Hospitals & Health Networks.
| Sidebar - Timing matters when planning security systems |
| Detailed planning of security systems with the appropriate parties prior to designing, building or renovating a hospital greatly can influence prices and satisfaction with the equipment. Many hospital security leaders say it's essential for them to be involved in the earliest stages of planning for hospital renovation and construction projects. But that's not necessarily what's happening, according to the 2011 Hospital Security Survey, which was conducted by Perception Solutions for Health Facilities Management and the American Society for Healthcare Engineering (ASHE) of the American Hospital Association and sponsored by Boca Raton, Fla.-based ADT Security Services Inc.'s Healthcare Solutions group. The survey found that while 60 percent of respondents said their hospital security department was involved in planning for security on most or all construction projects prior to breaking ground, 40 percent said security only was involved on some projects or not involved at all. While 59 percent said security was involved in the design stage and 21 percent at the preconstruction stage, nearly 20 percent said security was involved only at the construction stage or later. And only a quarter of respondents said the hospital security director makes decisions regarding the design and implementation of security systems in construction and renovation projects, while 58 percent said the facility's vice president or director makes the decisions. "It appears that some hospitals don't get security involved in the initial planning and design phase — sometimes they are not aware until a project begins," says Jim Stankevich, president of the International Association for Healthcare Security and Safety (IAHSS) and manager of health care security for Software House, Tyco International's security products division. "IAHSS has made a conscientious effort to make our members aware of the importance of their involvement from the initial stages of any design or construction project through IAHSS educational programs and seminars. The good news is our members are more aware and have become proactive in getting involved early on." Skip Smith, CHFM, SASHE, vice president of supply chain, clinical engineering, and facilities management for Catholic Health Initiatives and president of ASHE, agrees that security professionals should be engaged at the design stage in every construction project. "The majority of hospitals are doing that, but you want them engaged all along and consulted about the risks they see," he says. One large academic medical center had to tear down walls in its newly built facility to install appropriate security wiring because the security department wasn't brought in early enough in the design process, says Kevin Weeks, director of marketing for ADT Healthcare Solutions. "What I'm hearing is hospitals aren't engaging security until very late in the process," he says. That may be a function of how high security chiefs are in the hospital food chain. Forty-six percent of survey respondents said security reports to facilities management, 27 percent to the chief operating officer or vice president of operations, 7 percent to the CEO, 3 percent to risk management and 17 percent to other departments. "It all depends on where the security director sits in the administration," says Shane Meenan, director of health care sales for ADT-Advanced Integration. "In some hospitals where security is less progressive, security equipment is often specified or installed without the knowledge of the security department. But in most urban hospitals, for instance, security is a top administrative priority and a product or design would never be specified unless approved by the security director." |


