
2017 Salary Survey results

In the first 27 years of his career, Mark Robinson, CHFM, climbed the ladder from carpenter to maintenance supervisor but worried that advancement opportunities might end there without a college degree.
But when his supervisor at Tufts Medical Center, Boston, encouraged Robinson to seek a Certified Healthcare Facility Manager (CHFM) credential through the American Society for Healthcare Engineering (ASHE), it opened the door to other opportunities.
After earning his certification in 2012 and attending night school, he began pursuing an associate’s degree through a relatively new Healthcare Facilities Leadership program at Owensboro (Ky.) Community & Technical College.
The online program is built around the core CHFM disciplines and was developed in cooperation with ASHE and the Kentucky Society of Healthcare Engineers.
Robinson began classes in 2014 and earned his degree this summer. During that time, he landed an assistant plant director’s job at Massachusetts Eye and Ear in Boston and in 2017, he became director of the physical plant at New England Baptist Hospital, Boston.
“I don’t think I would have moved into either of these positions without the degree,” Robinson says. “There are very few associate’s degree programs for health facilities managers, so I was lucky to find this one.”
The hard work has paid off. In two years since he earned his degree, Robinson’s salary has increased by 50 percent.
In its fourth year, the program has awarded five degrees and one diploma, according to Program Director Mike Canales, a long-time facilities manager. There are 70-75 students from 30 states enrolled in the program, which is yielding impressive results.
“Every single graduate previously working in health care has been promoted or got the position they were after, generally as facilities managers, directors or supervisors,” Canales says.
Facilities salaries increase
In today’s complicated, competitive health care environment, education and certification are becoming critical not only to career advancement, but also to better salaries.
And while pay hikes may not be keeping pace with increasing responsibility levels, salaries for Health Facilities Management (HFM) readers are on the rise, according to a 2017 survey of management compensation conducted by HFM in cooperation with ASHE and the Association for the Healthcare Environment (AHE). The survey comprised 1,047 respondents — roughly 31 percent with more than 25 years of experience in health care.
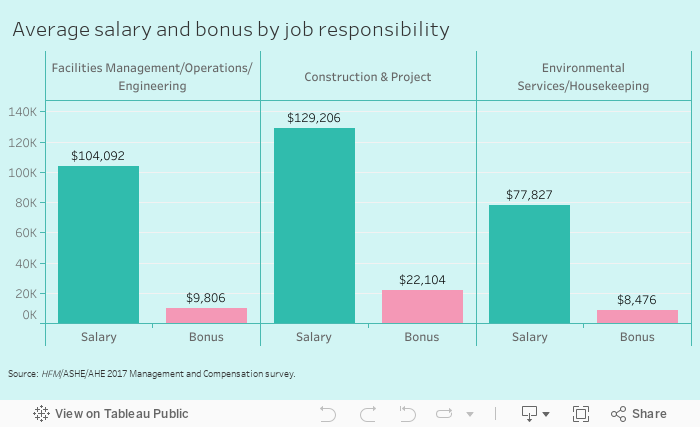
In the 2017 survey — the most recent HFM survey since 2015 — salaries for facilities management/operations/engineering increased by 5.2 percent to an average salary of $104,092. In the 2015 survey, facilities management/operations/engineering salaries increased by 3.4 percent to an average salary of $98,950.
“There is a pretty good market now because a lot of people are retiring and facilities managers’ roles are becoming more complex,” says Cheryl Harper, former director of building operations, Providence St. Joseph’s Hospital, Chewelah, Wash. “Qualified candidates are in a good position to negotiate higher salaries.”
Salaries for construction managers also saw a hefty increase, rising 9.4 percent from 2015 to an average salary of $129,206.
Environmental services (ES) salaries increased by 4.3 percent between 2015 and 2017, for an average salary of $77,827. Based on the 2015 HFM survey, ES salaries increased by 8 percent from 2012. But fewer ES managers participated in this year’s survey, which likely impacted the numbers, says Patti Costello, executive director of AHE.
“With the number of responses [being] lower than in past years, AHE is cautious about what is worthwhile data to report and what is not,” Costello says. “But I think it also speaks to how little time professionals have for extra activities and balancing work/home/family."
Health care drivers
Many of the factors driving salary increases are linked to larger shifts taking place in health care overall.
As health care becomes decentralized, facilities managers are inheriting a growing number of outpatient facilities. The pressure to keep budgets lean means they are being handed more duties and departments — heightening the need for education, training and certification. Simultaneously, baby boomers are retiring in large numbers, creating a shortage of qualified candidates to fill middle and top management positions.
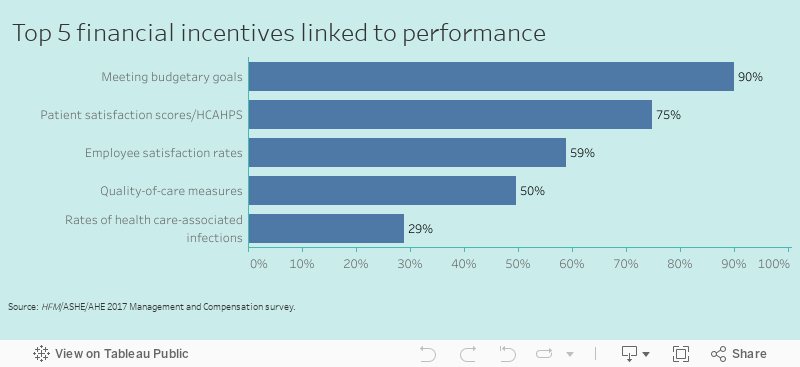
Roughly 54 percent of those surveyed said compensation is tied to performance initiatives and outcomes, with 90 percent naming budgetary goals as the top incentive. Though they scored much lower, two incentives new to the survey — employee satisfaction and employee retention — signal the emphasis hospitals are putting on keeping good employees.
“Hospitals are restructuring and are trying to stay lean,” Harper says. “It is more efficient to pay the employees you have better — to retain them and make them happy.”
Yet, facilities managers are absorbing an increasing amount of responsibility for the money they are receiving, the survey shows. Roughly 22 percent of respondents said the number of departments that report to them has increased, down slightly from a 27 percent increase in 2015.
“We continue to see the responsibilities of health care facility managers expand as the number of departments reporting up to facility managers increases,” says Patrick J. Andrus, CAE, ASHE executive director.
View more from the 2017 Salary Survey
Tim Adams, FASHE, CHFM, CHC, director of leadership development for ASHE, says facilities managers are not only taking on more departments — everything from security and safety to emergency management and food services — but also are managing more buildings.
“The days when one facility manager oversees one hospital are long gone,” says Adams. “Along with a primary hospital, a facility manager could be overseeing 50 or more outpatient facilities.”
In fact, the number of managers working at health care systems jumped from 20 to 36 percent, while those at acute care/general hospitals dropped from 63 to 53 percent, the survey shows. Those working at satellite offices — a new category in 2017 — is already at 11 percent, outpacing rehab and long-term care facilities.
Costello adds that ES managers also are being asked to take on more responsibility — in some cases, multiple disciplines over multiple facilities. “As ambulatory care grows and inpatient services decrease, there is a lot of shifting of internal staff,” she says. “The staffing models vary widely and geography plays a key role as well."
Education initiatives
To fill management vacancies, hospitals seeking qualified employees are relying more than ever on education and training initiatives to help employees with minimal education to move up the career ladder.
In 2013, when Paul Bugie began his job as system-
level director, facilities services/safety officer at Memorial Regional Health Services Inc., Belleville, Ill., he quickly launched in-house and off-site training programs, which have been well-attended in the past four years.
“Most of the power plant employees have finished the off-site training,” says Bugie, who oversees 31 full-time and one part-time employee. “It’s very hard for a solid mechanic to move up into management without some formal education.”
Tuition reimbursement, career ladder programs, mentoring and entry-level management training for qualified employees also were mentioned by respondents as ways to move up the career ladder. ASHE and AHE certification, conferences and resources were highly recommended throughout the survey.
“We budget for and encourage supervisors to take all of the AHE courses,” says Lea Beach, CHESP, T-CHEST, environmental services manager at Mercy Health in Janesville, Wis. “We require three courses per year from the AHE website.”
Said one respondent, “Certification is required for front-line staff, shift leads, trainers and department leaders.”
And some hospitals are mandating education. Said one: “Supervisor level and above are required to attend four leadership training courses per year.” Said another: “Mandatory 50 hours of self-improvement are required per year.”
Martin Wheatley, director of facilities for Owensboro Health Muhlenberg Community Hospital in Greenville, Ky., encourages his staff to pursue the health facilities associate’s degree at Owensboro (Ky.) Community Technical College, which will help to fill coming vacancies. “Senior leaders are looking for people to take our places once we start retiring,” he says.
Certification and salaries
Facilities and ES staff who are seeking higher salaries and career advancement have a golden opportunity through ASHE and AHE certification, which often translate into a substantial pay increase.
“As the survey results highlight, hospitals are recognizing the value a Certified Healthcare Facility Manager brings to their organizations,” Andrus says.
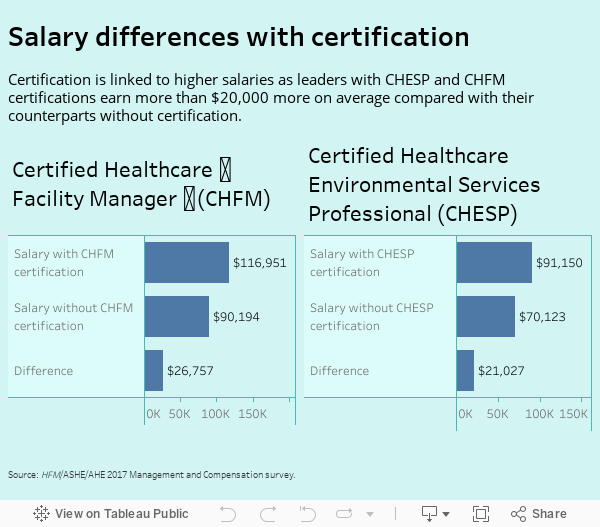
In a sample size of 634 respondents, facilities managers with this certification earn an average of $116,951 annually vs. $90,194 for those not certified. A sample size of 162 ES managers who are Certified Healthcare Environmental Services Professionals (CHESPs) earn an average of $91,150 vs. $70,123 without this credential. Certification also increases bonuses for facilities and ES managers.
While some hospitals do not mandate certification for new hires, credentialing is still on the rise for facilities managers. The 2017 survey shows that 34 percent have earned CHFM credentials, up from 25 percent in 2015. For ES managers, 7.2 percent have earned a CHESP credential.
Certification is definitely on the minds of leaders who recognize the importance these credentials carry.
“We are encouraging CHFM and CHC (Certified Healthcare Constructor) first, then we discuss advancing degrees with key individuals,” said one survey respondent. “We are adopting the CHEST (Certified Healthcare Environmental Services Technician) program for lead people.” Said another: “Management positions now require levels of formal education/certification.”
As health care and job responsibilities evolve and regulations become more complex, the need for certification will only increase with time, leaders say.
“The credentials will only gain in significance and recognition as the health care environment continues to change and delivery models become more complex,” Costello says. “The salary differential for a CHESP vs. a non-CHESP is significant and worth the effort.”

Planning ahead
Another factor affecting salaries is the aging of the health care management workforce and ensuing retirements. Succession planning — grooming talented people within and outside the facility to fill key vacancies — is becoming more critical than ever.
“Succession plans determine what leadership you have, when those people might retire and help you plan for recruiting and grooming people to fill those looming gaps,” Adams says. “That could involve education, training, mentoring over the next year … or the next five years.”
Although most facilities haven’t adopted a formal succession plan, the survey shows, many are beginning to put some type of plan in place. Said one leader, “There are two managers in place below me — one for the day shift and one for the night shift(s). The succession plan is having one or both of them ready to step up if I move on.”
Some facilities are taking new approaches to recruiting, such as partnering with local educational institutions to train top candidates for hard-to-fill positions. One facility is working with the local community college to create an internship program to train and recruit technical staff.
Most facilities do not yet have internship programs in place (just 17 percent, according to the survey), but leaders expect those numbers to spike quickly.
“Internships are a great way to bring a person in for a period of time to see how they work, how they fit in,” Adams says. “It’s almost like having a 12-week job interview.”
Hackensack Meridian Health’s Jersey Shore University Medical Center in Neptune, N.J., launched its internship program when a college student approached Chad Haraschak, resident regional manager, environmental services and patient transportation, about working in health care after graduating. “Her interest in sustainability filled a need of mine at the moment,” Haraschak says.
Working part-time, the paid intern helped with the facility’s patient experience program, wrote and rewrote program manuals and assisted with sustainability projects. It worked so well that Haraschak plans to expand the internship program to other students.
“The current intern has already expressed interest in coming back,” he says. “If interested in a few years, we plan to hire her full time.”
Employee retention
Finally, just as critical as recruiting good employees is retaining them, which also requires dedicated planning.
Hospitals are using strategies like career ladders, flexible scheduling, supporting certification, bonuses for performance, engagement surveys, and employee recognition and service excellence awards to keep patients satisfied. Higher pay and bonuses are always an incentive.
When the clinical engineering department at University of Rochester (N.Y.) Medical Center began losing valuable, junior-level technicians who were trapped in a system based on seniority, departmental leaders decided to revamp the program structure entirely.
After obtaining buy-in from senior management, leaders created a skills-based promotion system, codified training requirements and adjusted salaries. Since adopting the program, the department has been successful in retaining skilled junior technicians who previously couldn’t advance until a senior tech left, says Don DiVita, clinical engineering director at the medical center.
“We knew that investing money in training would go a long way in satisfying employees,” DiVita says. “We wanted to create an opportunity for people to grow and reduce turnover, which can be costly.”
Another facility is using retention bonuses so that employees who stay in the department for one year without any disciplinary action can earn an extra $2,000.
In the four years in his job, Bugie has seen a 20 percent improvement in employee satisfaction through less formal strategies such as potlucks, seasonal celebrations, gift cards and letters from the CEO, which work wonders in keeping employees happy.
“We have made significant efforts in employee satisfaction since I arrived here,” he says.
Developing such initiatives requires a considerable commitment of time and effort, but the payoff can be significant.
One respondent said, “Not only has our department been involved in the development of new employee engagement and retention programs, the entire organization has participated. We are focusing on engaging our employees. The happier and more satisfied they are, the better salesmen and women they become.”
Beth Burmahl is a Lisle, Ill.-based freelance health care writer.
Data for this report was collected and compiled by Jamie Morgan, associate editor of Health Facilities Management; and Suzanna Hoppszallern is senior editor for data and research at HFM’s sister publication Hospitals & Health Networks.
Related Articles

CMS data highlights opportunities to advance emergency preparedness
Here are the five most commonly cited emergency preparedness deficiencies at hospitals and tips on how to correct them.

The EVS professional's role in managing old and new pathogens
What environmental services departments should know about pathogens like measles and bird flu and how to stop their spread.

ASHE launches committee to help answer member questions
The new MyASHE Response Committee will work in coordination with the ASHE Regulatory Affairs Team to monitor and respond to critical questions.