
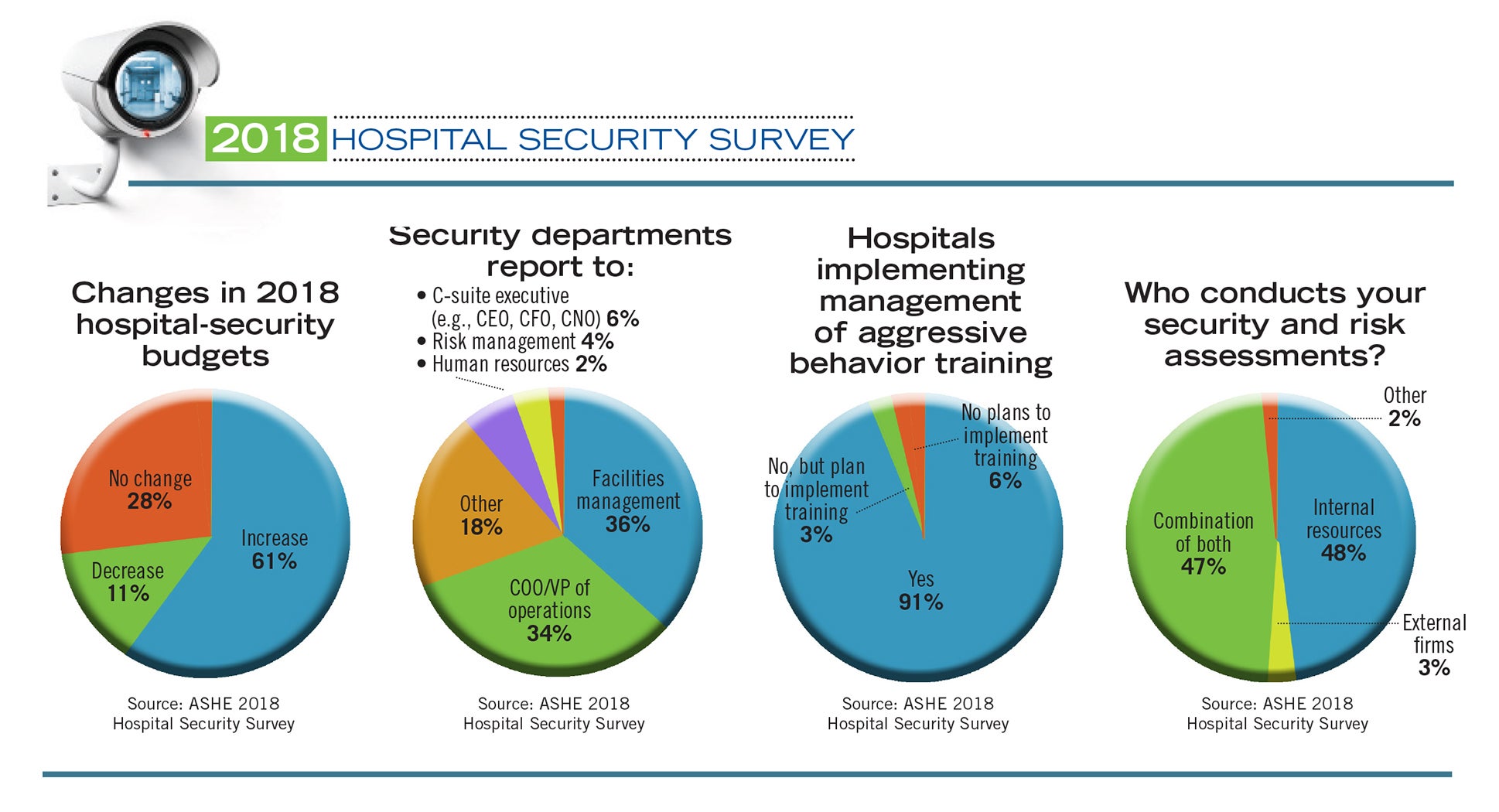
2018 Hospital Security Survey
More than half of American hospitals witnessed an increase in violence against staff over the past year, according to the American Society for Health Care Engineering’s (ASHE’s) 2018 Hospital Security Survey. But hospitals are responding.
This year’s survey, which was conducted in collaboration with the International Association for Healthcare Security & Safety (IAHSS) and completed by 315 hospitals across the United States, was the fourth such survey since 2011. It asked 32 questions in categories ranging from budgeting for security departments to technologies being deployed. While respondents represent a small fraction of the country’s approximately 5,000 hospitals, the survey provides a glimpse into security practices being adopted.
“While I believe we have made some important strides in improving security at health care facilities with improved polices, budgets and staffing as reflected in the survey, we can also see from the survey that we still have a lot of work to do,” says Jonathan Flannery, FASHE, senior associate director of advocacy for ASHE. “The good news is that organizations are seeing these as important issues and the more this happens, the more likely we are to reduce security risks to our patients, staff and visitors.”
Incidents rise
Hospitals see violence frequently, especially in the emergency department (ED), and this year’s survey showed that the number of these incidents seems to be on the rise. It is possible that some of the increase is due to more accurate reporting of incidents rather than an actual increase, but as shown in the data, 57 percent of respondents reported an increase in violent incidents against staff in the ED, and 52 percent saw an increase outside the ED. In the 2016 survey, those numbers were 51 percent and 44 percent, respectively.
Incidents of trespassing also rose in nearly half of the hospitals surveyed, up from 34 percent of hospitals in the 2016 survey.
But in all other categories of violence, many fewer hospitals reported increases. No hospitals reported an increase in infant abductions, for example, and 11 percent saw a drop in that crime.
How a hospital chooses to protect against risks should be based on a risk assessment, notes Kevin Tuohey, 2018 board president of IAHSS and executive director of research compliance at Boston University and Boston Medical Center.
“IAHSS recommends that risk assessments be done on a regular basis consistent with the review of policies at their facility,” Tuohey says. “Furthermore, IAHSS recommends that a root-cause analysis be done following significant events and a risk assessment following changes to the physical or operational environment.”
The survey showed that most hospitals are heeding that advice. More than 98 percent of respondents said they conduct risk assessments, and 72 percent do so annually.
There are many factors that go into a risk assessment, and hospital systems typically determine the risk of each facility individually, according to Bryan Warren, a former president of IAHSS and a national health care security consultant.
“You can’t base security decisions solely on square footage,” Warren says. “Size is not the only indicator. All things being equal, if I put one building in a high-crime area and another in a residential area, they are likely not going to suffer the same security issues. So it has to be looked at on a case-by-case basis, using objective characteristics like size, complexity and patient population to determine the security needs. It’s not cookie cutter.”

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mitigating the risk involves addressing the violence robustly, and nearly every hospital surveyed reported having a workplace-violence policy.
“We implemented a systemwide workplace violence-prevention program, which includes annual site visits for each department throughout the organization,” one respondent to the survey wrote. “The site visit consists of a group discussion with staff regarding their security concerns and a comprehensive physical security-hazard assessment of their work spaces. This program has allowed us to identify and resolve over 150 security-related concerns in less than a year after implementation.”
Controlling visitors
Controlling who is in the hospital is a key security tactic, and hospitals are taking steps to do that.
For example, every hospital surveyed this year either already has electronic-access control or plans to implement it in the next 24 months. The majority of hospitals also reported having video-surveillance systems, the ability to electronically lock down the hospital, and a panic alarm system.
However, only 42 percent of hospitals reported having a visitor-management system, which requires each visitor to sign in, provide ID or be photographed, and wear a badge. This level of control can deter unauthorized visitors because they must deal with a security person face-to-face.
One hospital system with which Warren is familiar recently implemented new visitor-control procedures at several of its primary facilities, he says. After normal hours, anyone arriving at these hospitals enters through a visitor-management point, where they are questioned about who they are visiting and given a temporary visitor pass. In some locations, visitors must provide a government-issued ID or have their photo taken.
“We have really focused on visitor management,” Warren says. “That’s been huge for us. If you can better control who’s on your campus, particularly after routine business hours, you stand a better chance of limiting problems. The people coming with the intention of committing a violent act will notice it’s a harder target — they’re getting badged, they’re having their photo taken, they see the video controls. So they go somewhere else.”
Controlling who is in the hospital is one of The Joint Commission’s Environment of Care standards, notes Karim Vellani, owner of Threat Analysis Group LLC, an independent security consulting firm that helps hospitals improve their security.
“That’s a difficult requirement to meet, and The Joint Commission doesn’t seem to be requiring that hospitals implement visitor-management programs at every entrance 24 hours a day,” Vellani says. “It’s a challenging effort, and expensive.”
Vellani, who chairs the research committee of the IAHSS Foundation, says that organization plans to publish a study on the efficacy of visitor-management systems in 2019.
Controlling visitors also means controlling what they bring into the hospital, and many respondents to the survey reported that they use metal detectors, either handheld or walk-through types.
Walk-through detectors, which require constant staffing and bag screening, are only in use in 11 percent of responding hospitals.
“Metal detectors are used to try to prevent weapons from coming into the hospital and, anecdotally, the majority of violence in hospitals is not committed by people with weapons,” Vellani notes. “So it’s not surprising that the use of walk-through metal detectors is low. They are expensive, and they can be a real challenge in multientrance hospitals.”
On the other hand, the increased use of handheld detectors — the percentage of hospitals that use them jumped from 33 percent in the previous survey to 50 percent in this survey — may imply that hospitals are focusing their efforts on at-risk individuals rather than the general public, Vellani says. That may be a more cost-effective way to deploy metal detectors.
The fear of weapons in the hospital has driven hospitals to take other precautions, too. Ninety-six percent of survey respondents have an active-shooter policy, up 1 percent from 2016.
“[We] created and implemented an active-shooter program wherein all new hires are introduced to the subject during employee orientation and then each unit is trained to run, hide or fight,” wrote one respondent to the survey.
Another respondent noted the risk of weapons in the emergency department: “[We are] in the process of implementing 24/7 weapons screening for our emergency department. As a Level I trauma center that services forensic patients, a homeless population, drug and alcohol addiction, and mental health [patients], weapons in our ED has become top priority in our risk management.”
The survey showed that the use of “man traps” jumped from about 13 percent of hospitals in 2016 to nearly 20 percent in 2018. These devices, which are a set of interlocking doors in which the second door cannot be opened until the first door closes, can be used to significantly slow down and/or keep out people trying to get into the hospital.
Tuohey notes that man traps may be worthwhile if a hospital’s risk assessment reveals that identifying high-risk populations is a priority prior to deciding about entry into the hospital.
“If you have a high incidence of problems that makes you think about how to protect your perimeter, then man traps might be an option to entertain,” Tuohey says. “But if you have low risk in that area, you may find that the man trap slows down your traffic significantly, without good reason.”
Budget and staff
The survey shows that hospitals are spending more on security and beefing up their security staffs. The survey also asked respondents what caused their budgets to change, and 56 percent said upgrades to their systems and staff and 50 percent said changes to risk level.
Those budgets will probably continue to rise, Tuohey suggests.
“Health care facilities need to attract good security staff and need to be at market rates to do so,” he says. “More importantly though, health care facilities need to invest in mitigating risks. [IAHSS] believes that the mitigation of risk through staffing, training and the growth of systems will continue to drive budget increases.”
Staffing is a challenge, though. Several respondents to the survey specifically mentioned difficulties in attracting good security personnel.
“Finding qualified candidates is becoming increasingly difficult,” one respondent wrote. “We have been forced to hire candidates that we would not have in years past, and this has resulted in its own set of issues.”
However, other hospitals have responded to the staffing situation innovatively.
About this survey
The American Society for Health Care Engineering and the International Association for Healthcare Security & Safety surveyed a random sample of 3,386 health facility professionals to learn about trends in hospital security. The response rate was 9.3 percent, or 315 completed surveys.
One survey respondent said his hospital set up its own training program for security officers: “We have developed our own in-house, state-certified law enforcement training center, which allows us to ensure that the training our officers receive is relevant. We have also partnered with police agencies in the areas where we have hospitals. This allows them to receive the training we provide, and [allows] our officers to gain commissions in those jurisdictions.”
Supporting security
Regardless of how a hospital addresses its security concerns, the issues should not rest solely on the shoulders of security staff, Tuohey says. Instead, security should be addressed collaboratively with the C-suite, other hospital departments and external resources.
“My message is that security issues need to be supported throughout the hospital,” Tuohey says. “Security staff can promote and provide expertise, but it is better received, budgeted and implemented when discussed, designed and delivered as part of a collaborative team process.”
Ed Avis is a freelance writer based in Chicago and Jamie Morgan is associate editor for Health Facilities Management magazine.
Related Articles
Preventing a possible outbreak through emergency response and remediation
Lessons learned from a real-life hospital flooding scenario and six steps for response.
Five things to include in a physical environment mitigation plan
A quick guide on how to identify and address physical environment issues quickly and effectively.

The facilities manager’s role in reducing healthcare-associated infections
From multidisciplinary communication to establishing safety procedures for construction, remediation and maintenance, facilities teams play a critical hand in reducing patient infections.