
Decontaminating high-risk patient settings

EVS staff are primarily responsible for ensuring a clean and disinfected health care environment.
Image by Getty Images
The health care environment includes not just solid surfaces, but also air and water. For each of these aspects, various departments must collaborate to ensure that correct processes and products are employed to reduce contamination and infection risk.
Environmental contamination poses the greatest risk to patients who are more vulnerable to infection such as those with suppressed immune systems and those with indwelling devices or surgical incisions, which create potential portals of entry for pathogens.
Sources of contamination
Following is a closer look at sources of environmental contamination and some key remediation approaches:
Air. Some pathogens are small enough that they can remain airborne for extended periods of time, such as Mycobacterium tuberculosis. For these infections, respiratory isolation and N95 respirators are required to prevent transmission beyond the index case.
It is also possible for larger particles such as skin squames (scales), laden with bacteria including methicillin-sensitive Staphylococcus aureus (MSSA) and methicillin-resistant Staphylococcus aureus (MRSA), to become transiently airborne when disrupted by air currents. Skin squames are constantly being shed, posing an infection risk in the operating room, especially for procedures involving an implant.
To minimize this risk, operating room engineering controls must be monitored and maintained within prescribed parameters. This includes air pressure, humidity, temperature and filtration. Adjunctive technology may be applied to further reduce contamination in the air for the highest risk surgical procedures. This includes mobile and built-in additional air filters, and combination high-efficiency particulate air filter plus UV-C disinfection.
Bacteria can also become transiently airborne during patient bed making in hospital rooms, especially when linen is not changed daily and may contain bacteria-laden skin scales and hair. This dispersion of bacteria poses a potential risk to patients with indwelling devices, which create a direct portal of entry to the vascular and urinary organ spaces.
The engineering or facilities department generally holds the responsibility for operating room air quality in collaboration with perioperative services. Reducing the risk of patient linen contamination during transport from contract laundry service and during use is typically a shared responsibility between environmental services (EVS) and nursing departments.
Water. Bacteria and mold can contaminate hospital plumbing surfaces (e.g., sink drains, faucets, shower heads and ice machines) due to any number of risk factors including stagnation, warm versus hot water temperatures and plumbing feature design. These pathogens can then be transmitted by hands, equipment and aerosolization to patients, increasing infection risk.
Generally, the patients affected by waterborne pathogens are those with compromised immune systems, or including those receiving immunosuppressive therapy. The bacteria most commonly associated with waterborne outbreaks is Legionella. Legionella water management programs are now standard for large buildings including hospitals in the United States.
Examples of chemical and physical control measures reflected in these water management programs include measurement of chlorine levels, maintaining prescribed temperatures in water heaters, avoiding stagnation in plumbing systems, regular maintenance or elimination of decorative fountains and monitoring of chemical levels in cooling towers.
In addition to Legionella, there are other waterborne pathogens that can cause patient infection. Contamination prevention for all waterborne pathogens involves a combination of engineering (e.g., avoid stagnation) and hygiene measures (e.g., routine disinfection of water features and handwash sinks).
Resources
Water safety requires a team effort typically led by facilities services, with consultative input from departments of accreditation and licensing, infection prevention, infectious diseases and risk/quality management. Of course, EVS staff are responsible in most hospitals for cleaning and disinfection of handwash sinks, toilets and ice machines.
Hard and soft surfaces. Bacteria contaminating surfaces in the immediate patient area (i.e., patient zone) creates a significant infection risk. Routine environmental cleaning processes are often suboptimal due to human factors such as inadequate training, resulting in incomplete removal of pathogens. This can lead to development of biofilm, which enables bacteria to survive for long periods and to develop resistance to common hospital disinfectant products.
A six-year study in four New York City hospitals published in the May 2018 issue of Infection Control & Hospital Epidemiology demonstrated that when a patient is admitted to a room where the previous patient was colonized or infected with a multidrug resistant organism, that patient has a 5.8 times increased risk of infection. This risk is directly related to insufficient cleaning of environmental surfaces.
The patient zone poses the greatest risk to the patient when contaminated because this area contains the surfaces that a patient may touch or may touch the patient.
Examples of patient zone surfaces include the bed, bed rails, privacy curtains, bed linen, bedside table, call bell, TV controls, bathroom sink and toilet, doorknobs and chairs. Also included is movable equipment, which may or may not remain in a patient room such as intravenous (IV) pumps, IV poles and bedside commodes. In addition, handheld devices such as personal and hospital-provided smartphones and tablets are being used with increasing frequency.
The pathogens that are causing the greatest concern in health care facilities today that can be transmitted by contaminated hard and soft environmental surfaces include Clostridioides difficile infection and MRSA as well as extended-spectrum beta-lactamase-producing organisms such as Klebsiella pneumoniae and Escherichia coli.
The EVS department is primarily responsible for ensuring a clean and disinfected health care environment. However, there must be collaboration among EVS, nursing and ancillary departments in determining accountability and ensuring the cleaning of all surfaces and items in the patient zone.
Reducing contamination
Over the past decade, the Association for the Health Care Environment (AHE) has led the way in guiding and training EVS technicians relative to reducing contamination on environmental surfaces, thereby supporting the goal of reducing infection risk.
The AHE training programs include a Train-the-Trainer course, permitting one EVS manager or technician to become trained and subsequently train their entire EVS department. This is a cost-effective and practical offering being leveraged by an increasing number of hospitals. Through AHE training and leadership, increased collaboration among EVS departments and other health care providers and ancillary personnel is fostered. The certification that accompanies the AHE training programs helps to not only increase the competence but also the professionalism and recognition of the critical role served by EVS technicians.
Innovative and improved cleaning products, chemicals, technologies and quality-assessment products have emerged over the past decade, adding to the arsenal of the EVS technician in support of infection prevention. These include microfiber cloths and mops, cleaning chemicals and disinfectant solutions with shorter contact times, quality assessment tools such as adenosine triphosphate (ATP) and fluorescent markers, and automated technologies that serve as an adjunct to manual cleaning, including UV-C disinfection and hydrogen peroxide vapor.
The evidence supporting these tools continues to grow. For example, in a multihospital randomized controlled trial, adjunctive methods for terminal cleaning procedures were studied. The findings, published in the Feb. 25, 2017, issue of Lancet, included a statistically significant decrease in organism acquisition by patients when adjunctive cleaning methods were employed to supplement standard cleaning processes, especially UV-C disinfection.
Remaining challenges
Not all hospitals have the resources to leverage the training and certification offered by the AHE and may not prioritize EVS product purchases, training and staffing in the hospital budget. Additionally, challenges remain with recognition, rewards and, consequently, retention of EVS staff in many hospitals. Often these critical health care partners are underpaid and underappreciated.
Compounding this problem in some locations is the practice of outsourcing EVS services. This sometimes creates a disconnect between cleaning practices and recommended cleaning standards, as the contract staff may have been trained for cleaning in a hospitality environment instead of a clinical environment.
In a hospitality environment, the population is generally healthy. In a clinical environment, the population is generally ill and with compromised immune systems and indwelling devices. The requirements and competencies associated with cleaning these environments are very different.
In addition, although designed to support reduced infection risk, innovative cleaning products, chemicals, technologies and quality assessment products all require EVS staff training to utilize them effectively. This is not always possible with a high turnover rate in the EVS department and lack of certified EVS trainers.
Although AHE offers standards for health care environmental cleaning, there remains a lack of standardization across U.S. hospitals. The results of a survey by N. Kenters et al. in the Oct. 2018 issue of The Journal of Hospital Infection that evaluated differences in hospital cleaning practices, points to insufficient EVS training as a primary reason for this lack of standardization.
The survey found that only 70% of facilities train EVS staff at time of hire; 46% received additional yearly training; 15% receive additional twice yearly training; and 20% receive sporadic training. For contact precaution rooms, 15% of survey respondents reported that no additional cleaning was required; only 9% reported disinfection was added to cleaning. The majority of respondents indicated that visual monitoring was the sole method for assessing the quality of cleaning.
As yet, there is no recommended minimum set of standards to guide selection and purchase of the various categories of environmental cleaning and disinfection products on the market.
A good example is microfiber cleaning cloths and mops. Science has proven that microfiber outperforms cotton cloths and mops, but there are so many types, it can be daunting for EVS departments to select the correct products. Not only are there reusable and disposable microfiber products, but some are impregnated with germicides, and some not. In addition, there are variations within each of those categories with regard to the qualities of absorbency, durability, dispersion and release, and cost.
The way forward
To support optimal patient safety, hospitals must ensure that a clean environment is a top priority. Fortunately for U.S. hospitals, AHE offers valuable resources for EVS departments, including cleaning standards, training programs and certification. These are fee-based, so EVS departments must ensure a budget sufficient to leverage these tools.
In addition, adequate staffing levels for hospital EVS departments is foundational to supporting the journey to zero preventable health care-associated infections. One facility management expert recommends that cleanable square footage, frequency of cleaning, lock-in areas and space classification must be considered when determining staffing levels for EVS departments. For more detailed information on determining EVS staffing levels, see the sidebar.
Two performance improvement stories illustrate practical pathways to optimizing EVS processes and outcomes, incorporating some of the same key focus areas.
In the first, an EVS optimization project was initiated by the San Francisco chapter of the Association for Professionals in Infection Control and Epidemiology in partnership with one local hospital.
Later, under the leadership of a different team, this project was enhanced and expanded to include a total of 10 hospitals. The project at all sites was guided by a performance improvement playbook, which can be accessed at www.zeroinfections.org/esop---evs-optimization-playbook.html. The playbook was designed as an easy-to-follow recipe focusing on key elements:
- Identification of an executive champion for the EVS department.
- Sponsorship of an EVS staff member to attend AHE training and return to train all staff in the EVS department.
- Collaboration between EVS and nursing departments in determining cleaning accountability.
- Development of a cleaning quality assessment program with frequent feedback to EVS staff and the infection prevention and control committee.
- Development of a recognition program for EVS staff.
At the conclusion of the three-month playbook project at the first hospital, an online EVS staff evaluation was done that reported improvement relative to multiple components of the EVS program.
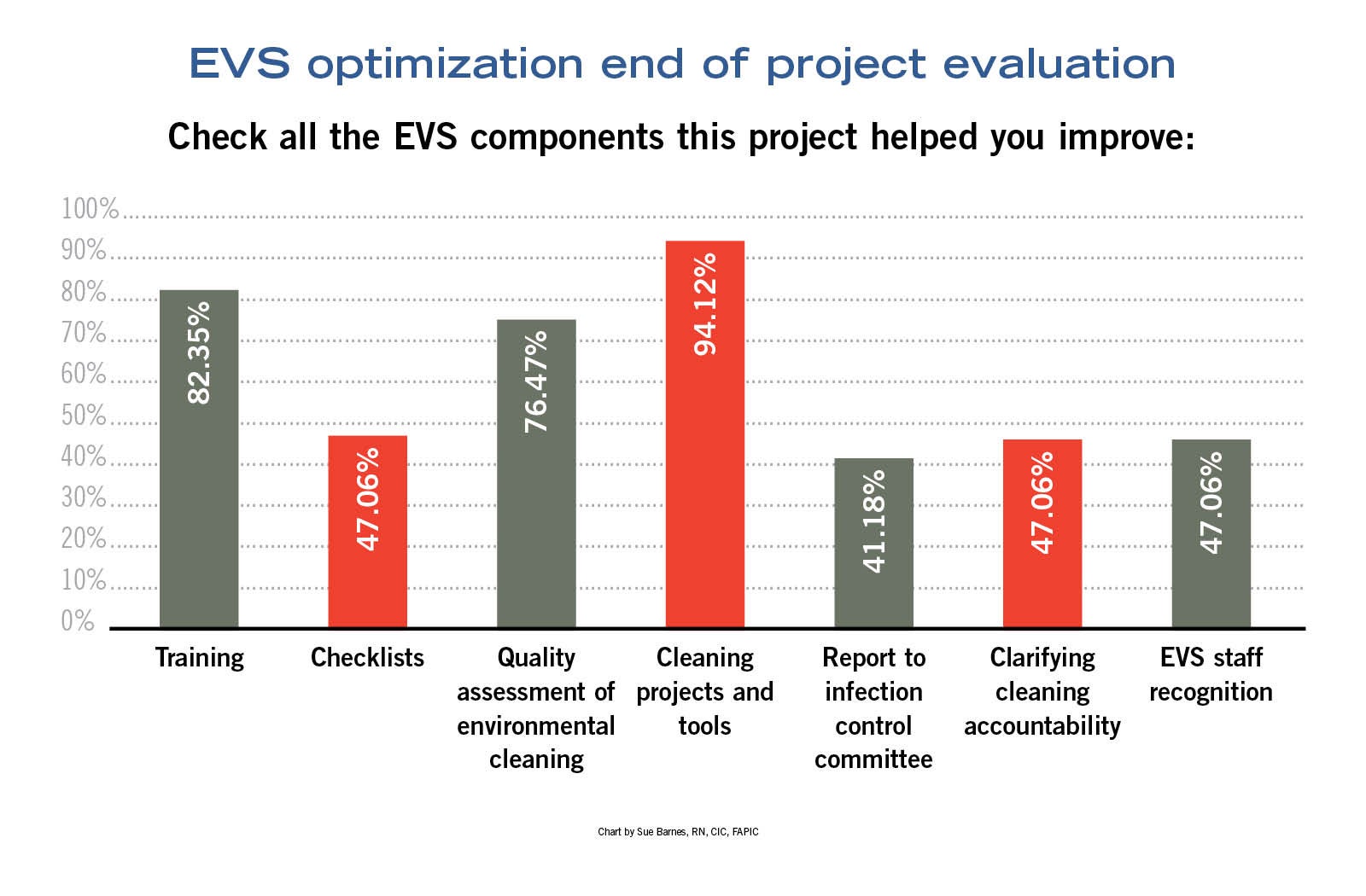{kind=link}
The post-project survey from the additional 10 hospitals is still underway in nine of the 10 locations. In the first survey returned to date, respondents report improved EVS staff morale and recognition, and successful introduction of fluorescent markers to assess cleaning quality. After three months, the fluorescent marker score in that hospital was 90%. Although the remaining post-project survey results are pending, anecdotal reports indicate improvements in the processes and outcomes of the EVS programs.
Using a different approach with some of the same areas of focus, an article by Allen et al. in the June 2018 issue of Infection, Design & Health described the creation and implementation of an EVS bundle over six months that included the following elements:
- Targeted training for environmental hygiene (including addressing cleaning roles and responsibilities, bundle requirements and local context).
- Defined and consistent product use.
- Availability of point-of-care wipes for medical equipment (i.e., nurse-cleaned items).
- Defined and consistent cleaning technique, including addressing sequence, friction and movement, and adherence to manufacturers’ instructions for product use, including contact time and dilution.
- Regular quality audits with results fed back directly to EVS personnel.
- Enhanced communication among EVS workers and other health care personnel.
- Hospitalwide promotion of environmental hygiene.
After bundle implementation, significant improvements in cleaning performance were observed, with an increase in fluorescent marker cleaning assessment scores from 61.1% to 95.4%. Improvements in both the knowledge and attitudes of EVS staff also were reported.
A crucial goal
Keeping hospitals clean is a crucial patient safety-related goal.
While progress has been made, EVS departments are still faced with challenges in many hospitals, including insufficient training, staffing and compensation.
Success stories have demonstrated that with training, collaboration and executive championship, EVS processes and outcomes can be optimized.
Sue Barnes, RN, CIC, FAPIC, is an independent infection prevention and control consultant based in San Mateo, Calif. She can be reached at sueabarnes@gmail.com.
Related Articles

The EVS professional's role in managing old and new pathogens
What environmental services departments should know about pathogens like measles and bird flu and how to stop their spread.

Preventing winter rodent activity in health care facilities
As temperatures drops and the risk of rodents spike, proactive prevention will ensure patient safety and operational compliance.
2025 EVS Department of the Year: Aurora Medical Center Sheboygan County
The EVS's team commitment to collaboration and cleanliness are helping to drive better patient outcomes.