
Designing the inclusive inpatient room

An entry view of the virtual reality patient room concept.
Image by HGA
Health care design communities are steadfastly focused on improving quality, safety, dignity and efficiency in acute psychiatric units. However, as the number of patients with comorbid behavioral health and medical conditions increases, there is growing realization that current room designs fail to meet the multiple needs of this unique population.
Given this mounting challenge, a broad mix of experts, including medical planners, architects, facilities planners, psychologists/psychiatrists, clinicians, nurses and researchers, recently set out to apply an evidence-based approach to creating a new room type — the next generation of universal/inclusive patient room designs — to safely accommodate integrated medical and psychiatric care in the inpatient environment.
Journey begins
During the first phase of this journey, the study team considered the current state of knowledge on designing patient rooms for behavioral health patients, staff and family members. A literature review revealed that few rigorous studies on behavioral health environments existed. However, there were two recurring themes in the literature:
- Threats to patient and staff safety in the designed environment arise from mobility and accessibility challenges as well as potential ligature points within the patient room, equipment and furnishings that can be used to inflict harm.
- Satisfaction and well-being among patients, their family members and staff are adversely affected by the absence of a calming, healing environment.
After the literature review was completed, a focus group was held with study team members to identify, define and rank critical-to-quality (CtQ) needs for the new patient room design. CtQ is a Lean concept in which critical operational, design or human experience attributes, necessary to produce a measurable quality outcome, are identified.
The objective of CtQs in the health care context is to create an environment that will support quality care delivery. The CtQs identified during the focus group are discussed in the section below. While they are specific to the project, they clearly reflect the Institute of Medicine’s (IOM’s) six aims of health care quality.
Design charrette
Next, a design charrette that included clinicians from major medical institutions, researchers and medical planners was held to discuss and sketch design interventions addressing the CtQs. The charette took place simultaneously in three HGA offices — Minneapolis, Milwaukee and Washington, D.C. — and participants attended both physically and virtually.
During the charrette, room design and the interplay between patient and staff needs were explored. Critical issues that needed to be addressed in any resulting room design were identified within the IOM’s six aims:
1. Improve staff safety. Staff safety is a priority, as staff members need to be able to protect both the patient and others if an event occurs. If a patient is deemed to be at high risk for self-harm or harming others, one-on-one observation by a sitter may be required.
{kind=link}
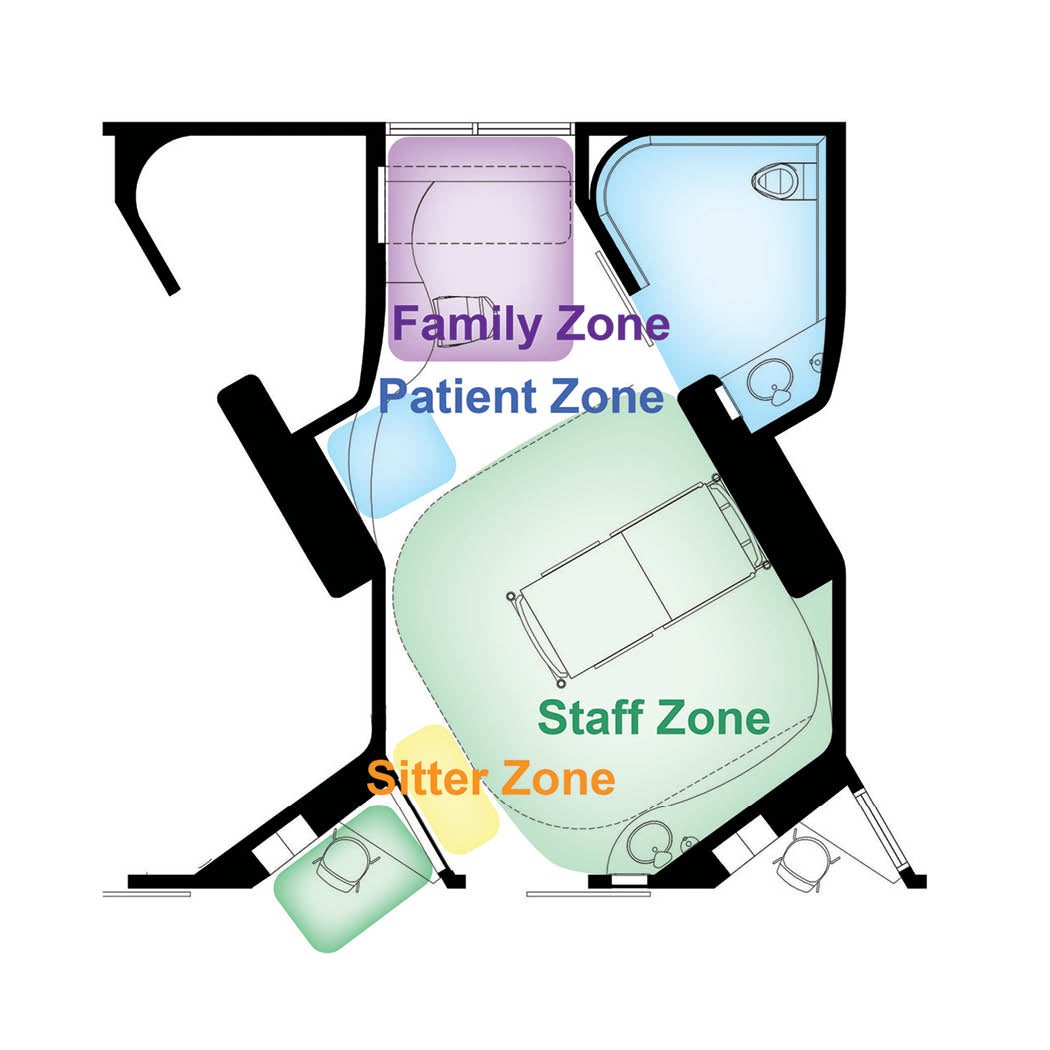
Priority needs to improve staff safety included a clear and consistent line of sight of the entire room, first means of egress for staff should an incident occur in the room, no hiding places and no opportunity for patients to use any room equipment or furnishings as a weapon against staff. Clear definition of a designated staff zone consisting of spaces for charting, hand-washing, storage, headwall and area for a sitter were provided within the patient room design.
Placing charting and observation space outside the patient room meant that, when staff were at the computer, they were always able to have eyes on the patient. Identifying an improved sitter location was based on similar needs: to facilitate surveillance of the entire room and having first means of egress. Curved angles and hidden, pull-out equipment and furniture throughout the room greatly reduced the risk of room components being used as weapons to harm staff.
2. Improve patient safety. Charrette results to improve patient safety focused on providing acuity-adaptable/universal room attributes (to eliminate the need to move patients to other rooms, which, in turn, reduces handoffs and medical errors), flexibility in patient bed-type (e.g., a hospital bed versus a platform bed, depending on acuity), reducing self-harm/suicide through anti-ligature room elements and minimizing the risk for falls.
The combination of medical and behavioral health comorbidity presents a challenge in terms of the patient bed selection. While there are currently “anti-ligature hospital beds” available on the market, many behavioral health experts consider them unsafe and avoid using them due to potential ligature points. As a result, medically fragile behavioral health patients requiring a hospital bed can be at increased risk for self-harm. In these cases, the ability of staff to observe patients is crucial.
Standard swing doors, showerheads and bathroom fixtures represent significant ligature risks in traditional medical-surgical patient rooms. During the charrette, special attention was paid to anti-ligature items such as patient-safe sliding doors and a continuous, patient-safe grab bar in the toilet room.
While the jury is still out on the best location for the toilet room to reduce the risk of falls in all types of patient rooms (e.g., on the footwall or the headwall), patients with medical and behavioral health comorbidities are often at additional risk for falls. Commonly prescribed anti-psychotic and anti-anxiety medications often affect equilibrium and balance. For this model room design, the decision to include an outboard patient toilet was based on the desire to enhance staff visibility into the toilet room.

The patient zone view of the virtual reality patient room concept.
Image by HGA
3. Increase patient and staff satisfaction. Charrette participants identified several ideas to increase patient and staff satisfaction. Broad categories included patient privacy, access to nature and daylight, patient control of the environment, calming and noninstitutional spaces, and cleanliness of the room. There was frequent overlap between patient and staff satisfiers.
{kind=link}
Single-patient rooms with private toilets significantly increase patient satisfaction among all types of patient populations. This is especially relevant for patients with medical and behavioral health comorbidities. For example, private rooms can enable patients with anxiety to reduce stress and control levels of stimulation. Patient control of room lighting and temperature also increase satisfaction.
The orientation of the patient bed (foot of bed rotated at a 45-degree angle to the corridor), combined with the placement of the charting station near the door, enabled staff to see the entire room (including the toilet). These features were thought to contribute to satisfaction among patients and staff. For patient benefit, visibility of staff can help patients feel they are being cared for and not alone.
Built-in/hidden equipment and an exterior window to access daylight and nature created a calming, noninstitutional environment in the proposed model room. Room cleanliness, identified as particularly important to behavioral health patients, according to some charrette participants, was enabled by the curved lines of the room (including walls, casework and counters), as there were fewer places for dust and debris to gather.
4. Provide family-centered care. Family-centered care in the comorbidity patient room was facilitated by lockers at the charting station where families could lock up their belongings before entering the room. The dedicated family zone in this design included a desk and a fold-out wall bed over the window bench, which could be seamlessly revealed as needed. Discussions during the charrette highlighted family egress concerns at this location when patients were at risk for harming others or were agitated. Options to safely accommodate family members on the other side of the room (near door) will need to be developed for these patients’ families.
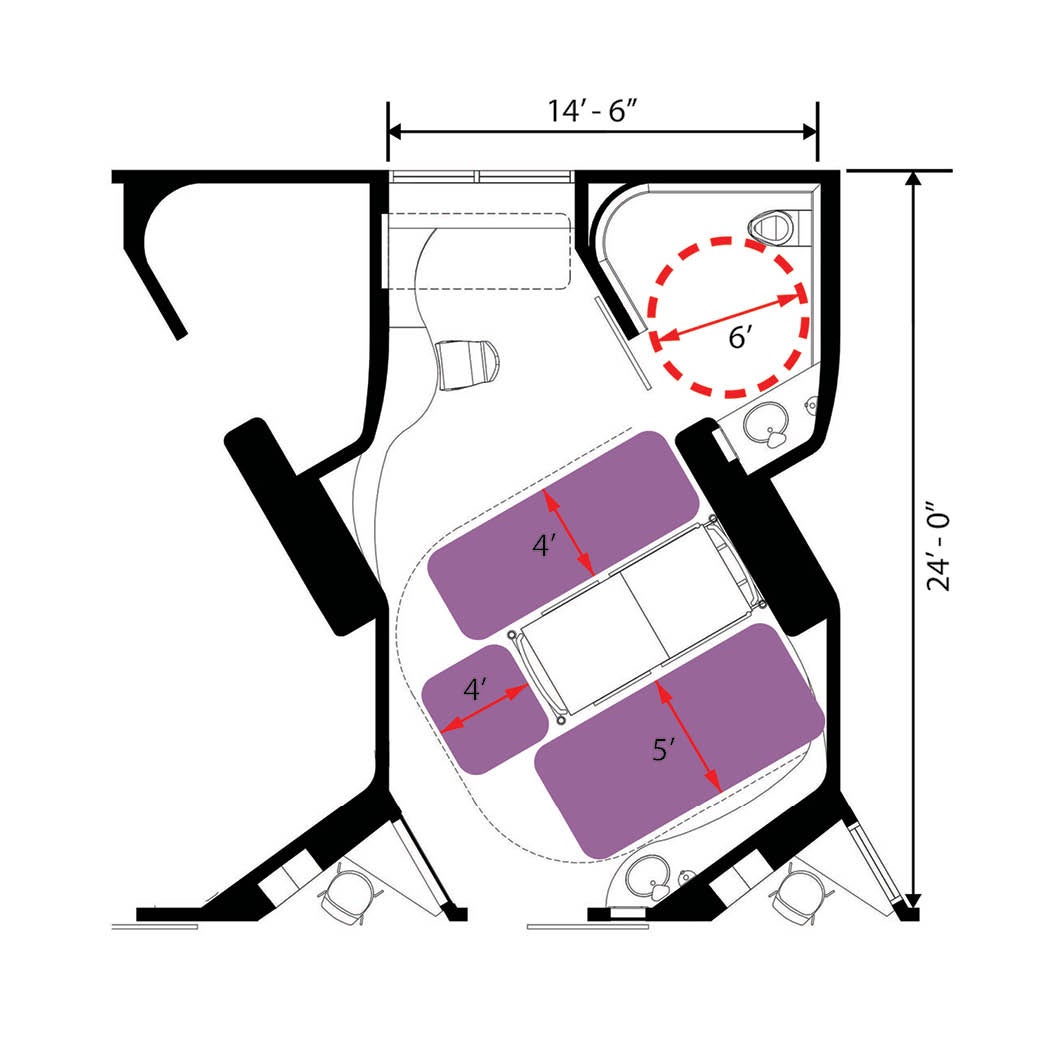
5. Increase staff efficiency. Decentralized supplies and equipment availability within the room as well as medication storage were identified by charrette participants as important features to increase staff efficiency. Safe places to store items within the room included a thicker headwall area and locked servers. Clearances provided in the model room work for any type of acuity and patient size: 5 feet on the transfer side of the bed (typical of an intensive care unit room), 4 feet at the foot of the bed and 4 feet at the far side of the bed. Toilet room clearance was set at 6 feet to be inclusive of all patient types as well as requirements for staff assistance.

The staff zone view of the virtual reality patient room concept.
Image by HGA
6. Create a healing, calming environment. Patient room windows to provide access to daylight and outdoor views, wall art, a television/information wall and privacy afforded by single-patient rooms were included to reduce stress and create a healing environment.
Animation and survey
Design solutions discussed during the charrette were turned into a preliminary room animation. The aim of the animation was to create a virtual patient room to evaluate prior to any construction. This allowed testing of the design elements and how they might be implemented. Feedback on the design was solicited and revealed problems associated with the location of the hand-wash sink. Upon entering the room, staff turn away from patients to wash their hands.
Other suggestions included providing a sink outside the bathroom to reduce a blind spot and repositioning the bed to provide a direct view out the window. While all these changes may not be possible due to other priorities, the virtual reality (VR) room was robust enough to gather valuable insight from participants.
An online survey was created for distribution to charrette participants and a few of their contacts. Question development was based on the findings of the focus groups and design charrette. Questions focused on the CtQ needs identified by the participants as they applied to the patient room design. Of the 15 people who participated in the survey, approximately 70% were female architects between 35 and 49 years old. After viewing the fly-through video, 77% of the survey participants reported being satisfied with the overall size and layout of patient, family and staff zones; bathroom and shower spaces; and the location of the hand-washing sink.
More than three-quarters of participants (81%) were satisfied with visibility in the patient room model, and 86% were satisfied with patient safety features of the room. High satisfaction (90%) was reported for staff features including nurse servers for supplies, a nursing alcove outside the patient room, and the suitability of the patient room design during both an acute behavioral health crisis and an acute medical crisis (e.g., a code).
Next steps
The next steps in the process will be to revise the design for future implementation based on additional VR experiences and questionnaire feedback. Application of the patient room design at the unit level also is planned.
As work with health care organizations that have behavioral health beds continues, data will be added to the study using the techniques described here. Additional charrettes will be organized to solicit feedback during health care design conferences, especially those focused on behavioral health.
A key ingredient in the success of this project was building a study team comprised of a broad mix of expert medical planners, clinicians and researchers. Additionally, the steps and outcomes of the evidence-based design approach — including a literature review to identify relevant design concepts, followed by focus groups to identify and rank critical-to-quality measures and needs for patients, staff and families — were crucial in helping the team to understand the impact of user needs on room design during the charrette.
By testing the resulting design in a virtual environment and soliciting feedback via questionnaires, progress is being made in creating a new room type. The study’s findings provide a unique opportunity to address the need for integrated inpatient medical and psychiatric care that will improve outcomes and better meet the specific design needs of this unique patient population.
Moving forward
As the team begins to apply the design in upcoming projects and solicit feedback from peers, they hope to collectively move the health care field forward on this important issue by helping to inform future Facility Guidelines Institute Guidelines references.
Shary Adams, AIA, ACHA, EDAC, LEED AP BD+C, is principal and senior medical planner; Terri Zborowsky, R.N., EDAC, CPXP, is design researcher; Kara Freihoefer, NCIDQ, EDAC, LEED ID+C, is director of research and associate vice president; and Lou Ann Bunker-Hellmich, EDAC, is design researcher at HGA. They can be reached at SAdams@hga.com, TZborowsky@hga.com, KFreihoefer@hga.com and LBunker-Hellmich@hga.com.
About this article:
This feature is one of a series of articles published by Health Facilities Management in partnership with the American College of Healthcare Architects.
Related Articles

ED expansion plans will advance care, enhance flow
Renovation will bolster capacity for the Baton Rouge, La.-area Level 1 trauma center.

Planning care spaces for daylight and views
New entries in The Center for Health Design's Knowledge Repository further the case for windows in patient care rooms.

Advocates for those who enter our facilities
The Center for Health Design's President and CEO, Debra Levin, contemplates the far-reaching impacts of health care facility design — and the responsibility that entails.