
Working in real time
Imagine a hospital in which patient beds and stretchers are always available when a patient is admitted and wheelchairs are found at the drop of a hat. These seemingly simple scenarios are being realized at many hospitals, especially those that have implemented real-time location systems (RTLS).
RTLS comprise various tag technologies, platforms (e.g., network appliances like readers, exciters and other components like servers, middleware and the location engine) and end-user software, and come in many different forms with many different applications. While RTLS exist in some health care facilities, it is more common that hospitals have evaluated this quickly evolving technology but have yet to act on it.
Why are some hospitals cautious about RTLS while others are optimistic? Hospital decisions often are based on whether implementation can achieve cost-savings. But it is also true that many hospitals have looked at the potential process, risk and care improvements that RTLS may provide and moved forward.
RTLS benefits
Most hospitals initially begin considering RTLS for asset management, where there are obvious nursing and clinical engineering benefits. For instance, if a nurse needs to find an available infusion pump, RTLS can help find one quickly. This is amplified in code situations when a device may need to be located in an emergency. Likewise, clinical engineers reap the benefits when searching for equipment that is due for preventive maintenance (PM). This helps to improve environment of care requirements for monthly medical equipment PM compliance.
There are other potential benefits throughout the hospital as well.
During the day, for instance, the available supply of wheelchairs at the main entrances of the lobby and in the emergency department (ED) often is depleted. RTLS can help alleviate this supply problem by passively monitoring when wheelchairs are taken from alcove areas. RTLS can then alert patient transport staff that more are needed when a certain minimum level is reached. While this may be considered inconsequential, not having a wheelchair available when a patient arrives can have a significant impact on patient satisfaction and Hospital Consumer Assessment of Healthcare Providers and Systems scores.
Similarly, unit-based staff adherence to tracking and logging temperature and humidity ranges as required for specimen refrigerators can be less than optimal. When ranges are exceeded, the logs often have no indication of action taken. If a hospital is audited for participation in Centers for Medicare & Medicaid Services (CMS) programs, inspectors from a CMS-approved organization go first to a facility's logs and often can cite the hospital for improper monitoring when follow-up actions are not noted. An RTLS can remove the human element in this process by measuring temperature and humidity continuously.
Finally, patient beds sometimes are piled up in a bed repair shop and additional ones are rented to meet capacity needs. Often, however, sufficient numbers of beds are available for use, but they are not well-managed. Implementing a system can help schedule repairs in a timely fashion and may help to minimize bed rentals. Additionally, this may apply to bed surfaces for specific clinical applications, especially in pediatric hospitals. RTLS can help to cut down on rentals of other clinical equipment, too.
Key planning questions
How do health facilities professionals select the right system for a hospital? RTLS involve interdependent technical considerations and the facilities department should be involved in determining what criteria will be used to drive the decision. Some key questions to ask are:
- What specific clinical and business problems need to be addressed immediately and what can be addressed in the mid- and long terms?
- What RTLS tags, platforms and end-user software are needed to meet these objectives?
- What degree of spatial resolution is needed to achieve these objectives?
- Is there proven interoperability between the system under consideration and other management systems that may be necessary to achieve the objectives?
With regard to interoperability, the system's end-user software application will need to be integrated with other systems to achieve improved workflow and maximum benefit. Systems that may need to be integrated with RTLS include:
- enterprise systems like admission/discharge/transfer, bed management, electronic medical record and billing systems;
- clinical information systems supporting such areas as radiology, laboratory and EDs;
- building and security systems;
- communication systems such as cellphone carriers;
- computerized maintenance management systems for clinical and facilities engineering.
Also, health facilities professionals will want to explore purchase strategies in conjunction with their information technology and supply chain programs. Generally, there are three approaches to vendor selection when acquiring a system: choosing the tag-and-platform vendor first, choosing the end user software vendor first or choosing to pursue vendors that only offer a comprehensive solution.
If the tag-and-platform vendor is selected first, facilities professionals will need to consider whether it also offers end-user software. If it doesn't, a separate vendor will need to be selected. On the other hand, some tag-and-platform vendors that offer software only will offer asset tracking and possibly temperature monitoring software; currently, most vendors do not usually offer workflow-related software. So, if the hospital wants to incorporate system information into a workflow process, it will need to focus its search on providers of comprehensive solutions or engage another software vendor with workflow functionality.
However, if the software vendor is selected first, the vendor may not offer the tags or platform. Rather, it likely will have a partnership with one or more vendors that offer the infrastructure components. End-user software vendors may present a fully integrated solution by partnering with their preferred tag-and-platform suppliers or they may offer consultative services to help the hospital decide which tag-and-platform vendor is most appropriate. In either case, it is important to marry the capabilities of the tag-and-platform solution to the needs of the application and pay particular attention to terms and conditions that ensure that all vendors are invested in collaboratively resolving any issues that may arise.
All about money
While there are many good process improvement reasons to implement RTLS, a hospital chief financial officer still will want to see achievable cost-reductions and not just the idea of saving time. Many of the potential hard cost-reductions associated with RTLS, such as improved inventory turnover times and decreased expired consumable products, will originate in the supply chain. Others, such as improved device availability and subsequent lower rental rates, will show up in the facility's departmental budget.
The up-front cost for RTLS is not trivial and hospitals can expect to see a wide range of prices. According to Plymouth Meeting, Pa.-based ECRI Institute's SELECTplus pricing database of capital medical equipment, the price for a particular asset tracking scenario — a 300-bed, hospitalwide implementation with room-level resolution, tracking 3,000 tags — could range from $100,000 to $2 million, depending on the type of tracking technology.
Among the most common types:
• Radio frequency (RF) systems are less expensive options and offer flexibility in terms of tracking. A 300-bed hospital with 3,000 tags choosing to utilize RF tracking can expect to spend from $100,000 to $275,000. This price includes the software, which covers licenses, subscriptions and service agreements, as well as the price of installation and other hardware.
• Wi-Fi systems are more expensive than RF systems, but slightly less expensive than the Ultra Wideband (UWB) systems. This often makes Wi-Fi systems an attractive alternative for many facilities. Wi-Fi utilizes the existing wireless network in a facility and additional access points to support the extra traffic. The main advantage to a Wi-Fi real-time tracking system is that the facility can track all medical devices, plus any other object that transmits an 802.11 signal, such as laptops. A 300-bed facility with 3,000 tags purchasing a Wi-Fi system can expect to spend between $300,000 and $650,000.
• UWB systems are generally the most expensive tracking technology. In fact, a 300-bed hospital with 3,000 tags choosing to utilize UWB tracking can expect to spend between $875,000 and $2 million. However, UWB systems offer advantages over other types of RTLS, such as a more robust signal transmission and a more efficient battery system. UWB also offers the ability to track very fine resolutions, allowing a facility to easily track multiple objects within a small area. UWB technology is recommended if facilities desire long battery life and precise location tracking.
The prices of these technologies can vary greatly depending on a number of factors including the differing sophistication and capabilities of the software, whether the end-user software and tag-and-platform are purchased as a turnkey solution and the basis for the cost (e.g., the license could be based on the number of tags, number of users or another quantity).
Factors that should be compared in the negotiated agreements include preinstallation consultation fees (e.g., workflow analysis), purchase price of the end-user software application, licenses for the software application, maintenance and software agreements, service costs, costs associated with interfaces to other systems (e.g., operating room scheduling system and computerized maintenance management systems), costs associated with ongoing software customization (e.g., creation or modification of software rules and reports), and clinical and technical training.
It is also possible that some vendors will enter into risk-sharing agreements with a hospital. In these cases, the vendor and hospital determine what the return on investment (ROI) should be over time. Based on specific and mutually agreed-upon stipulations, the vendor will share in the financial risk should the system not provide the expected ROI according to a predetermined schedule. Alternatively, the hospital may want to consider including financial incentives or penalties in its purchasing agreements to provide a level of assurance that the selected product will function as expected.
Implementation challenges
There are many implementation challenges to a system installation.
One of the first hurdles to successful implementation is a common nomenclature for all tracked devices. Wheelchairs are easily referred to as wheelchairs, but what about a refrigerator-freezer combination? In a good number of asset lists, many of these will be misclassified as just refrigerators or just freezers. Nursing staff often refer to heating pads as K Pads while clinical engineers refer to electrosurgical units as "Bovies." Asset names should be clarified and standardized to make a common listing of tracked devices. (The use of a formal naming convention in databases has many downstream effects as well.)
A critical variable for RTLS implementation is the physical layout of each hospital unit. The location of readers and signal exciters, cable trays, wireless infrastructure and electromagnetic interference concerns all must be assessed before implementation and re-evaluated throughout the process. The type of RTLS technology (e.g., ultrasound, radio-frequency identification or ZigBee) selected may depend on the hospital's physical layout.
Also important is determining the level of positional accuracy that is required. Wheelchair supply can be loosely followed through the use of a choke-point monitor at a defined geographical space. But another level of specificity is needed to determine the exact location of critical equipment, and the greatest level of positional accuracy is needed for patient-specific caregiver interactions if the hospital is trying to capture charges associated with discrete patient-care activities.
Another best practice is that one person be given the responsibility to maximize the system's use. RTLS easily can be deployed in less than a week at most hospitals; some vendors say it is even less time with their tags and trackers. But, while the physical installation may take less time than expected, perfecting the actual use of the system may not be so quick. Improperly resourced RTLS deployments may flounder with few process changes being implemented or goals achieved. Hospitals that have implemented RTLS successfully and changed care patterns and support services have appointed employees with wide-ranging operational, environmental and clinical knowledge to develop RTLS applications at their facility.
Improving operations
Every hospital looking at RTLS applications should identify what challenges might be overcome through its implementation. Whether it's tracking hand-washing compliance, maintaining PAR levels of catheters in the cath lab and interventional radiology suites, tracking Xbox consoles or finding facilities equipment that is part of a research grant's annual audit, the opportunities for RTLS to assist with improving hospital operations and care are almost endless.
Robert Maliff is director of applied solutions at ECRI Institute, Plymouth Meeting, Pa. He can be reached at rmaliff@ecri.org.
| Sidebar - How one hospital is planning for the future of health care |
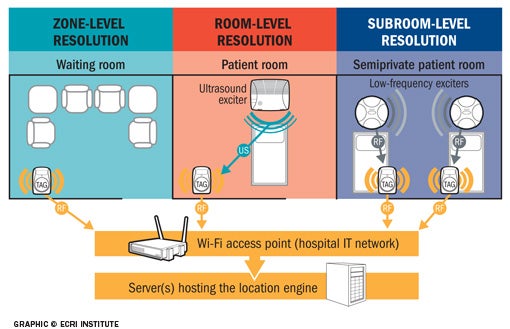
When implementing real-time location systems (RTLS), hospitals need to understand spatial and temporal resolution. Spatial resolution determines how narrowly a system can physically pinpoint an asset or a person's location and it has proven critical in determining the overall effectiveness of a system implementation. Spatial resolution is categorized in the following ways:
The more precise an object's location needs to be pinpointed, the greater the resolution required. For example, if the clinical engineering department needs to find a medical device to perform preventive maintenance, a zone-level resolution is likely sufficient because little urgency is involved. However, if a clinician needs to find a medical device for immediate use on a patient, then room- or subroom-level resolution will be needed. For any application that involves automating processes with tag-to-tag interactions, subroom-level resolution likely will be required. Temporal resolution determines how quickly a system can relay the location of assets or people to reflect their position in real time. Temporal resolution depends primarily on the beaconing rate (e.g., how frequently a tag emits a signal). Because assets do not move as frequently as people, tags affixed to assets may not need to send a beaconing signal more than once a minute. Conversely, a tag attached to a patient or staff member may need to send a signal every second or every few seconds. Latency in processing signals or information may affect temporal resolution. For example, the middleware location engine may require time to process vast amounts of data due to a large number of tags or frequent tag transmissions, as when tracking a moving individual. Also, because RTLS location engines need to interface with other systems such as the admit/discharge/transfer system for work optimization or for automated process monitoring and documentation applications, latency may become increasingly important. Computing systems are capable of handling massive amounts of data and likely will cause few problems for asset-tracking systems and most other applications, but as RTLS technology matures, more advanced applications are implemented and more data are exchanged with other systems, temporal resolution will need to be assessed. |
Related Articles

Health system invests millions in high-tech beds
NYC Health + Hospitals' upgrade marks a systemwide enhancement to patient comfort and care.

Agencies issue eight principles for OT cybersecurity
U.S. and international agencies released eight principles to eliminate cyber vulnerabilities in operational technology.

NFPA report reviews risks associated with smart buildings
The NFPA's Fire Protection Research Foundation report dissects the impact of smart building technology on life safety and presents a roadmap to address its challenges.