
Strategies to rebuild rural health care facilities
Click image to enlarge
There are over 2,000 rural hospitals spread across the U.S., and more than 20% of them are currently at risk of closure.
According to the University of North Carolina Cecil G. Sheps Center for Health Services Research, 170 rural hospitals in 33 states have closed since 2005, a trend that is accelerating, as at least 10 hospitals have closed each year since 2013. The financial risks and pressures are even greater now in the wake of the COVID-19 pandemic.

{kind=link}
Rural hospitals face a variety of challenges, including competing for highly sought-after talent graduating from medical schools, maintaining economies of scale, investing in capital and new technologies, and declining population in the areas that they serve. Recruitment is particularly challenging, as rural hospitals compete against the amenities major cities offer.
One successful strategy used by MidMichigan Health, Midland, Mich., is to open a family medicine residency, which provides more flexible training than a traditional internal medicine pathway and convinces many graduates of the program to stay with the health system. Because of relatively low patient volumes, specialists often are recruited to serve in several different facilities and rotate their days in different hospitals and clinics.
Rural hospitals are vital resources that serve as the primary safety net for almost one in six Americans, or more than 52 million people. Of those people, according to Kaiser Health Network, nearly 11 million live in a county with no hospital, and another 18 million have a hospital but no intensive care unit (ICU) beds.
This article centers on rural hospitals that are not critical access hospitals.
Importance of rural facilities
While some of the benefits of rural hospitals may seem obvious, it is worth outlining why they are so important to maintain and strengthen. The key to a rural health network, as stated by MidMichigan Health, is the ability to deliver “appropriate care close to home.”
Many emergency conditions, such as heart attacks, strokes, and complications associated with labor and delivery, are time sensitive, and a matter of minutes can dramatically impact the likelihood of patient survival. Rural communities may be located hours from the nearest hospital with specialized care, and the inability to get to timely care results in many preventable deaths.
Beyond emergency situations, limited access to routine care for dealing with chronic conditions reduces the likelihood that patients will maintain care regimens. According to the Centers for Disease Control and Prevention (CDC), patients in rural communities are more likely to die of all leading causes of death, including chronic causes such as heart disease, cancer, chronic lower respiratory disease and stroke.
Building rural facilities
Major capital projects can be daunting undertakings for smaller organizations, but there are key components that can improve the success rate and impact of construction within a rural hospital.
Strategies that can assist rural hospitals include the following:
Advancing profitable service lines. One key component is to start with profitable service lines that add to the hospital’s revenue and can fund future upgrades. While surgery, imaging and cancer treatment are expensive construction projects to undertake, state-of-the-art facilities and technology can help recruit surgeons and clinicians to increase volumes. They may also draw patients to the hospital who might otherwise travel farther to a different facility for elective care.
Procedural spaces, such as endoscopy, are also vital for an aging rural population. Procedure rooms can be co-located with surgical suites to share resources and allow for flexible staffing. Instrument processing and sterile supplies can be located to support both the surgical and procedural spaces. In some cases, depending upon schedules and caseloads, the operating rooms may provide excess capacity for the procedure rooms.
Surgical and procedural spaces should be designed with maximum flexibility so they can be used for a wide variety of case types with minimal changes in equipment and supplies. Investments in building systems and technology, such as surgical booms, new lights, improved HVAC and increased emergency power systems, can improve the care process, which gets patients home sooner and reduces the risk of infection or readmission.
Similarly, pre- and post-operative spaces should be designed to flex back and forth throughout the day, allowing a smaller footprint to support the same patient volume. A compact plan, with good visibility of patients, will provide for an efficient staff workflow.
{kind=link}
Click image to enlarge
Investing in flexible clinics. Basic clinic space that is flexible and adaptable to a wide range of uses is important to support rural health care. Many rural communities do not need full-time specialists in cardiology, orthopedics or neurosciences, but they do need access to these services.
Properly sized and equipped exam rooms can serve family medicine and primary care needs, as well as rotating specialty services and telehealth needs. Exam rooms should be equipped to meet basic needs in every room, with dedicated supply carts and equipment located nearby that can be wheeled in for each specialty on different days. Telehealth technology in the room, including PCs and digital cameras, enable the local caregivers and patients to connect directly to specialists anywhere in the world.
Careful attention should be paid to the support spaces of the clinic, as well. Consulting rooms are vital to supporting patient education and can double as telehealth spaces. Group consulting or education spaces can support classes to help patients deal with chronic health conditions.
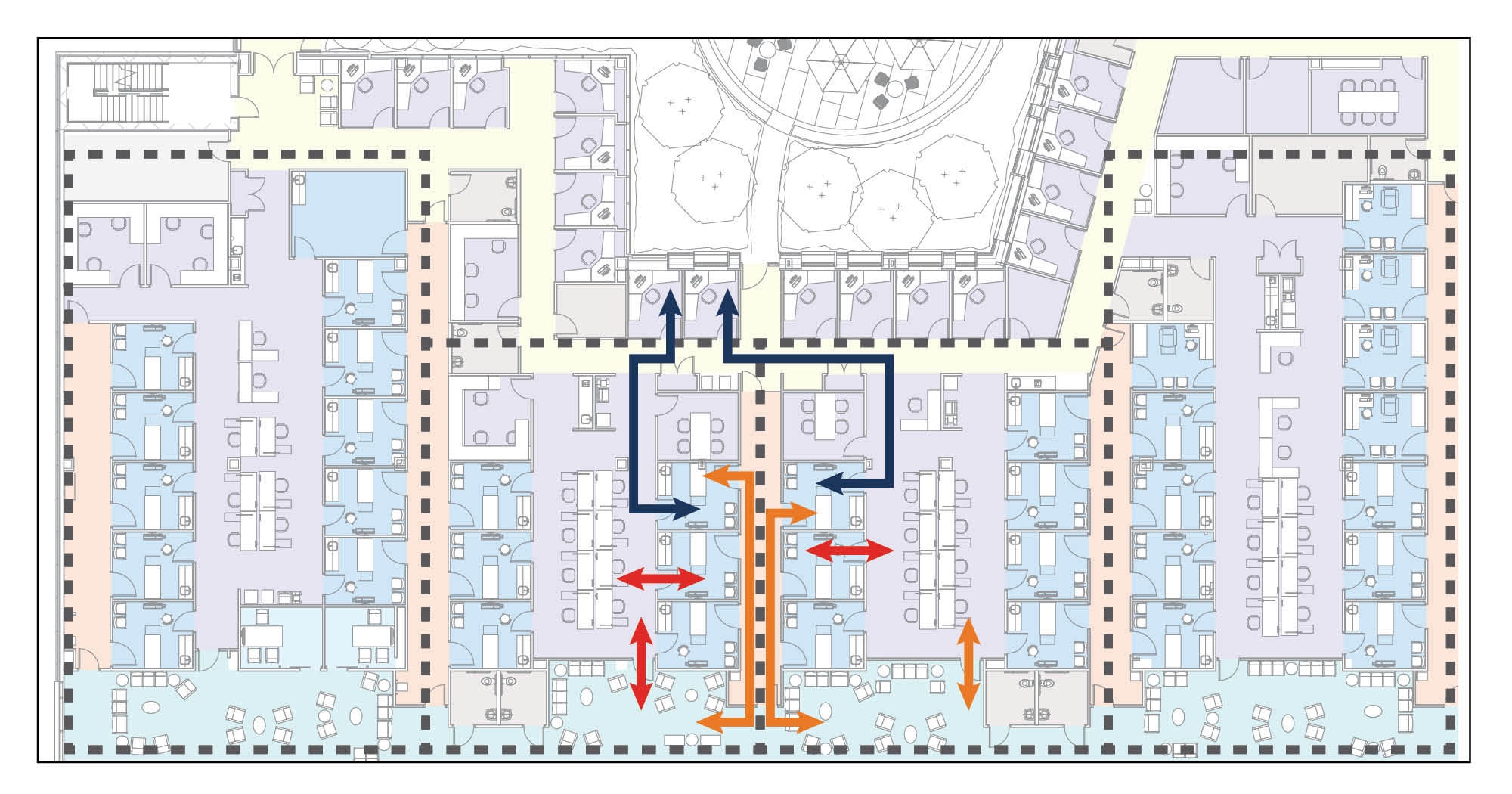
In addition, flexible staff work areas allow rotating specialists and their support staff who travel with them to have a home base during each rotation. The two-sided exam room model can be particularly effective in this situation, as it provides off-stage collaboration space for clinicians to coordinate care regimens without being overheard by patients.
{kind=link}
Click image to enlarge
Behavioral health can be integrated within the rural health clinic as well. Embedding these services inside of flexible clinic space provides easy access for primary care providers to refer patients with a personal handoff to behavioral health specialists. Initial introductions can be made in the exam room during a medical visit if the physician determines that the patient should be seen.
Integrating the services together can reduce the stigma that makes some patients reluctant to seek out behavioral health treatment.
Providing chronic care close to home. Another key area of investment is repeat services and treatment for chronic conditions, where patients may not be willing to travel as far frequently. Bringing these services close to the patient’s home is key for encouraging long-term patient health. Fortunately, these services generally are not as expensive to build either.
Rehab requires recurring visits, and long drives to centralized facilities will reduce the likelihood of patient compliance. Access to rehab before surgery is also linked to better outcomes and reduced recovery time, especially for joint injuries — one Mayo Clinic study showed that by doing rehab before surgery, patients returned to their sport 20% faster than those who did not go through the program.
Rehab spaces are relatively easy to add into an existing rural facility — the size of the program can be flexed based on the volume of patients to be served, and the equipment is not complicated. Rehab spaces can also be opened after hours to hospital staff or communities for general fitness to increase utilization and develop wellness habits.
{kind=link}
Click image to enlarge
Key design considerations are to provide large open spaces for flexibility, lots of natural light and views to nature, and good staff visibility of the gym space. Separation between general fitness use and clinical space needs to be considered if it is opened to the general public.
Other chronic conditions may require slightly specialized spaces that are vital to maintaining patient health. Dialysis and infusion therapies require frequent patient visits that require significant patient travel time to and from centralized services. More than 20% of all patients requiring dialysis live in rural areas, so providing care sites close to these patients is important.
Additionally, many patients suffering from other chronic conditions, such as heart failure, require frequent infusions or in-person visits to specialty clinics to manage their condition. In one recent study, managing atrial fibrillation (AF) patients through a specialized AF clinic measurably reduced the incidence of hospitalizations and stroke.
Developing flexible solutions and multi-use spaces. One of the keys to successful rural health care construction is maximizing the use of spaces by making them flexible. As noted previously, clinic space design can accommodate a wide range of specialties. In addition, other areas such as observation rooms can meet a wide range of needs.
Observation rooms can be used as overflow for the emergency department (ED), prep and recovery, or even extended post-surgical stays that don’t require an inpatient bed. If they are located adjacent to both surgery and the ED, they can flex back and forth between the services. In this case, they must have the utility support to meet both uses, including power, medical gases and HVAC systems, and they need good visibility from a nurses station. Should the rooms also be used for overnight stays, consideration can be made for access to patient toilets as well as appropriate privacy and lighting for sleep and recovery.
Inpatient rooms need to be flexible as well to handle a wide range of acuities. Most rural hospitals have basic medical-surgical capacity but some may require intermediate care and ICU levels of care. These may be needed infrequently, such during an outbreak of COVID-19 in a community, but it is important to design the systems into the building in advance to support the need should it arise.
Consideration for room size, equipment placement, HVAC, medical gas and emergency power should be provided so that some or all of the patient rooms can flex acuity in an emergency. Some rural hospitals may not have the staffing to support higher-acuity patients, so supplemental services may be provided remotely via telehealth. Providing technology support both in the room and at the nurses station to enable remote patient monitoring is important to enable this added support. By providing flexibility in levels of acuity, patients can be cared for closer to home, with more family involvement.
Some hospitals also may find that sharing resources with other organizations best leverages resources to provide appropriate care close to home. Easy examples of this are specialized imaging such as magnetic resonance imaging, nuclear medicine and positron emission tomography-computed tomography, all of which can be provided in mobile trailers. A dock on the outside of the facility allows two or three hospitals to share a mobile imaging unit that can be scheduled to visit each facility every week as needed to accommodate patient volumes.
Other intensive spaces, such as sterile processing, can be combined into a single off-site facility to serve multiple hospitals. However, care must be taken in planning to account for the expenses and logistics associated with the transport of instruments to and from the facility, and the potential need for surplus instruments and supplies due to extended turnaround times.
Replacing rather than recapitalizing. Most hospital facilities are maintained for decades, with ongoing projects that renovate or expand one piece at a time. Replacing an entire hospital can feel like a massive undertaking for any organization, but often it is the most appropriate and economical solution.
Many older facilities simply do not have the infrastructure to support renovations, including the size of the central plant and the floor-to-floor height to accommodate current code-required HVAC systems. Additionally, renovations in place can be more costly due to phasing and operational challenges of maintaining patient care around construction.
A replacement facility also may provide an opportunity to reimagine the model of care. An existing structure and the need to phase construction will inherently constrain design options, whereas a new facility allows the clinical team to reconsider everything from arrangement of departments down to details like patient-to-nurse ratios, medication preparation and surgical instrument processing.
Depending upon when the hospital was built and changes in demographics, some hospitals may need much smaller footprints in a replacement facility than they have in their current building. Finally, the availability of land in a rural community may make it cheaper to consider a new facility than a similar project in a more densely populated area.
A vital component
Rural hospitals provide routine and critical care in local communities to tens of millions of Americans across almost every state and are a vital component of our nation’s health care system.
Strategies such as those discussed in this article are effective ways to help rebuild rural health care facilities.
ABOUT THIS ARTICLE: This feature is one of a series of articles published by Health Facilities Management in partnership with the American College of Healthcare Architects.
Jim Albert, AIA, ACHA, LEED AP, is principal at Hord Coplan Macht, Baltimore, Md. He can be contacted at JAlbert@HCM2.com.
Related Articles

ED expansion plans will advance care, enhance flow
Renovation will bolster capacity for the Baton Rouge, La.-area Level 1 trauma center.

Planning care spaces for daylight and views
New entries in The Center for Health Design's Knowledge Repository further the case for windows in patient care rooms.

Advocates for those who enter our facilities
The Center for Health Design's President and CEO, Debra Levin, contemplates the far-reaching impacts of health care facility design — and the responsibility that entails.