
A preventive approach to the physical environment

The way to ensure everybody is on the same page is to understand the reason why negative outcomes occur.
Image by Getty Images
Health care facilities professionals often are busy putting out figurative “fires” that prevent them from planning for potential problems. However, health care organizations must redouble their efforts at managing the physical environment through a proactive and preventive lens.
Creating, implementing and overseeing sustainable, preventive action processes in advance of adverse events will not eliminate all negative outcomes, but it will minimize them. The concepts discussed here can help health care facilities professionals move from an “after an event” to a “before an event” mindset.
Formalized processes
The goal of a hospital is to provide the best possible patient care and, ultimately, save as many lives as possible. Moreover, formalized processes are required to reach the best possible outcomes for this patient care.
A health care organization cannot effectively and consistently provide the best possible patient care without having established, agreed upon formalized processes that ensure everyone is on the same page about what they are going to do before they do it, while they do it and after a process is completed.
Providing the best possible patient care doesn’t involve only clinical staff, medications and therapeutics.
Optimal outcomes are difficult to expect if the physical space and environment are not properly managed and maintained as well. This includes not just the infrastructure itself, but the facility’s equipment and the overall environment of care.
One of the biggest challenges in any organization, especially a hospital, is effective forms of communication. Regardless of the size or scope of an organization, how do facilities professionals ensure that everyone is on the same page? The way to accomplish this is to understand the reason why negative outcomes occur. It is almost always because of a lack of a process, a broken process or ineffective communication.
To achieve compliance with the Centers for Medicare & Medicaid Services (CMS) physical environment condition of participation (CoP), a hospital is required to determine how the condition of the physical plant and the overall hospital environment is developed and maintained in a manner that the safety and well-being of patients, visitors and staff are ensured.
Facilities professionals should start by clarifying what the physical environment consists of. In the health care setting, terms have been used to reference the physical environment such as “the environment of care” or the “seven sisters of the environment of care.” This description includes, but is not limited to, life safety management, safety, security, hazardous materials, emergency management, medical equipment and utility management.
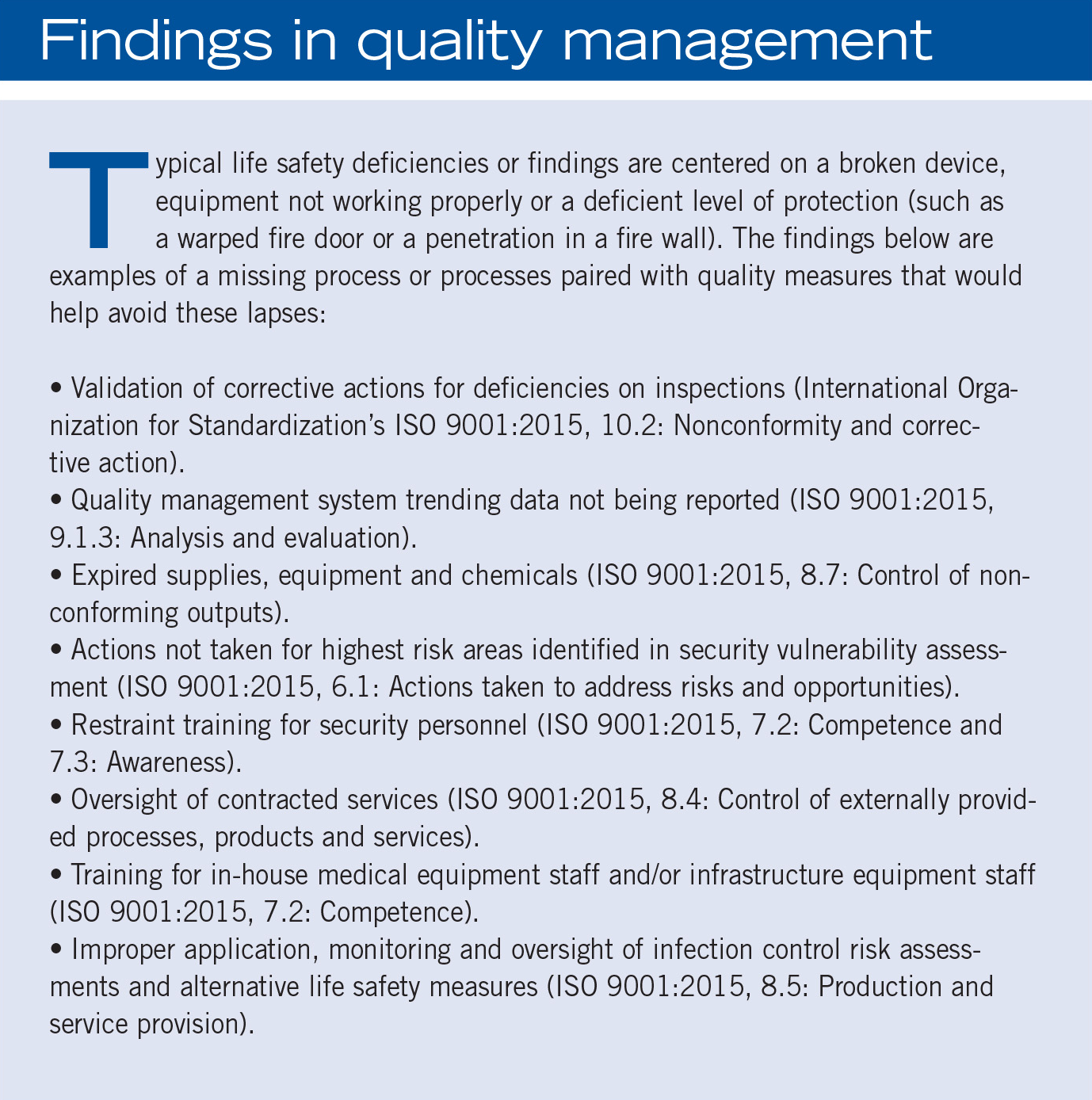
How do facilities professionals manage the overall physical environment and all the aforementioned areas effectively using a risk-based quality management system approach to eliminate, or at least mitigate, negative outcomes? This can be accomplished by combining the quality management concepts of planning, preparation, resource allocation, corrective action(s) and evaluations for effectiveness with concepts of the identification, prioritization, impact evaluation, mitigation and elimination of various forms of risk and applying them to the physical environment.
Begin by determining the scope of the organization specific to the physical environment. Considerations should be given to identifying the appropriate facilities manager and what they do. What are the expectations? Once these are understood, facilities professionals can develop formalized processes related to the required areas of the physical environment, and anything else specific to what the facilities professional does.
For example, security management is a requirement for all hospitals. Facilities professionals should perform a risk assessment to determine what type of formalized processes may be necessary specific to security. A security vulnerability analysis may determine the necessity to have armed security officers or certain high-risk patient populations housed in areas that have locked doors (such as pediatrics or behavioral health units).
Using a risk-based mindset, the next question that arises is: Does the organization utilize existing staff that are trained internally, a contracted service or local law enforcement? Hospitals are allowed to determine the who, what, when, how, why and where they manage security in their facility as long as they have effective processes in place to ensure a secure environment.
Another example could be for utility management for medical gas maintenance. Piped medical gas systems are required to be maintained per the original equipment manufacturer’s guidelines. Does that mean the manufacturer or a contracted service has to perform the maintenance? It is not always clear.
The 2012 edition of the National Fire Protection Association’s NFPA 99, Health Care Facilities Code, 5.1.14.2.2.5, will allow a health care organization to qualify their own staff member(s) to perform inspections and preventive maintenance if certain criteria are met. As with security management, if the utility management system is effectively implemented and maintained, it will meet the CMS CoP for the physical environment.
Conversely, examples of formalized processes that are not necessarily required for all hospitals would be how to manage confined spaces, hot work processes, or even industrial power truck training if forklifts or power jacks are present (these may or may not apply). The Occupational Safety and Health Administration’s OSHA CFR 1910.146 — Permit-required confined space, defines, outlines and gives direction on general environmental controls to manage permit-required confined spaces in general industry, if they exist.
By performing a confined space evaluation, the hospital determines whether confined spaces are present, how they are classified and how they are going to be managed by the individual facility in terms of access control, work performed and safety protocols that are required to oversee if or when work is performed in these areas.
The scope of this process may include hot work permitting, monitoring of hazardous gases, determining whether safe entry and work conditions exist, and any other miscellaneous hazards that may be present. (To learn more about confined spaces, see the Compliance+Operations article in the July issue of Health Facilities Management.)
How do health care facilities professionals know if the formalized process is working the way it is intended? What is the step-by-step process of ensuring the consistency of the desired outcome? Utilizing the plan-do-check-act (PDCA) cycle is one of the most effective formalized processes that can ensure consistent end results. It provides a simple and effective approach for solving problems and managing change and risk.
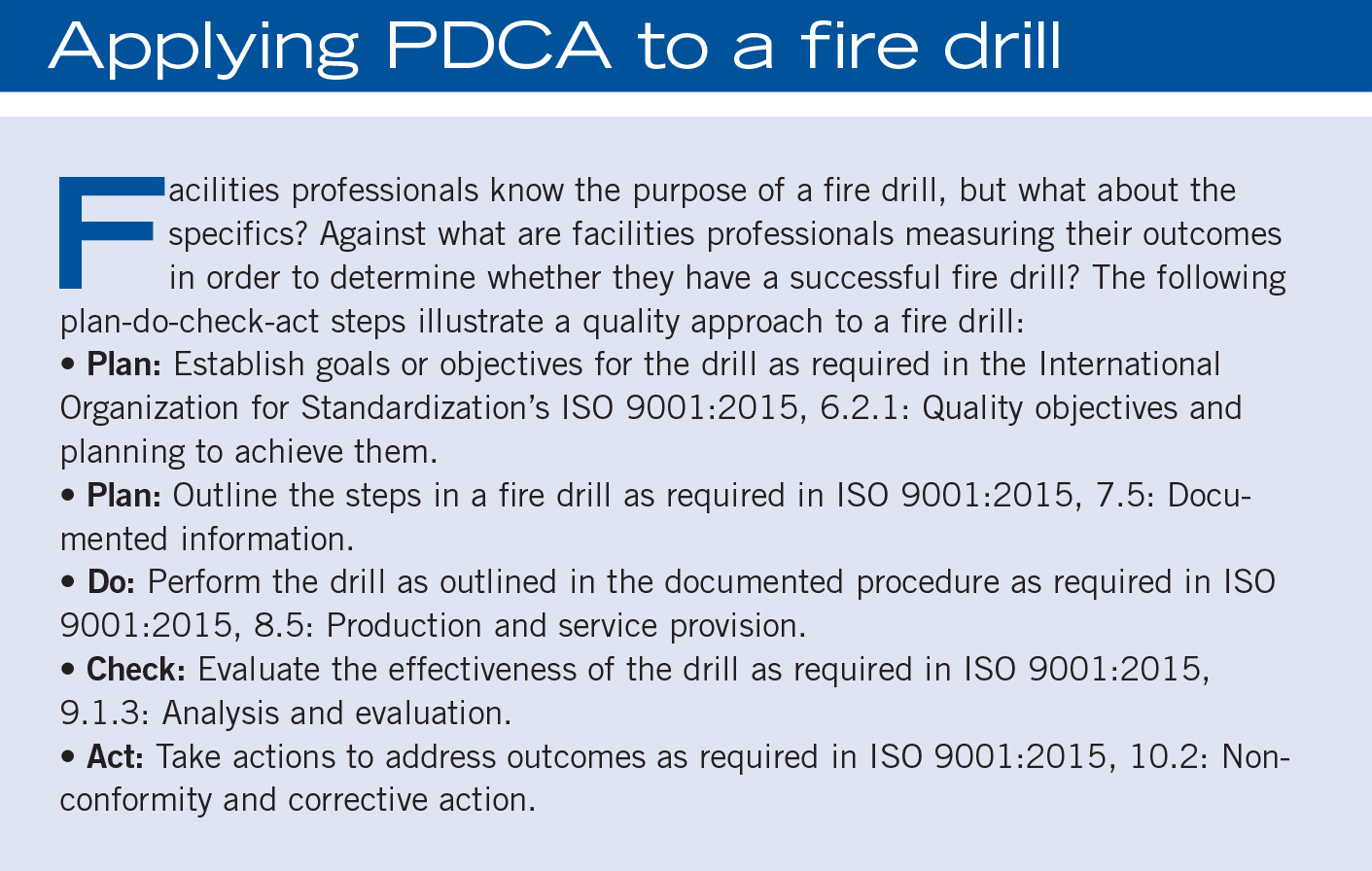
One of the more common examples of a continuous loop, or repeated process, in the physical environment nationwide is a fire drill. Fire drills are “planned” out based on not only known requirements from NFPA 101, but also using a risk-based approach to determine where, when and how to conduct the drills.
Once the drills commence, staff perform or “do” the planned process, and observing staff can “check” to make sure the planned and agreed upon process is conducted as originally designed. Upon completion, the observers evaluate and determine not only whether the agreed upon processes were followed, but they also identify what worked, what didn’t work, and what changes are needed to “act” upon before conducting another fire drill in either the same area or another location within the hospital.
This concept repeats itself again and again over time to determine consistency in this preventive action process. The whole point of conducting fire drills is to “practice the plan” so if an event occurs, staff communicate and perform their actions and duties in the most efficient way to ensure the highest chance of preventing injury to patients, staff and other visitors who may be present. The PDCA cycle allows organizations to formalize any process they want while acting as a guide to ensure key critical elements are not overlooked or missed.
Resources and competency
In health care, a significant amount of focus is applied around ensuring that clinical staff are properly trained. This includes, but is not limited to, licensures, certifications, training programs and regular evaluations of performance specific to the clinical realm of patient care. However, this is less frequently a focus regarding the physical environment.
It is very important that hospitals properly credential doctors, nurses and ancillary clinical staff. An untrained medical professional, especially in an emergent event, can mean the difference between life and death. All things considered, a health care organization can acquire the world’s best talent in terms of clinical staff, medications and therapy, and the latest technology to take care of its patients, but the reality is that all of this will be limited if the lights go out.
Resources
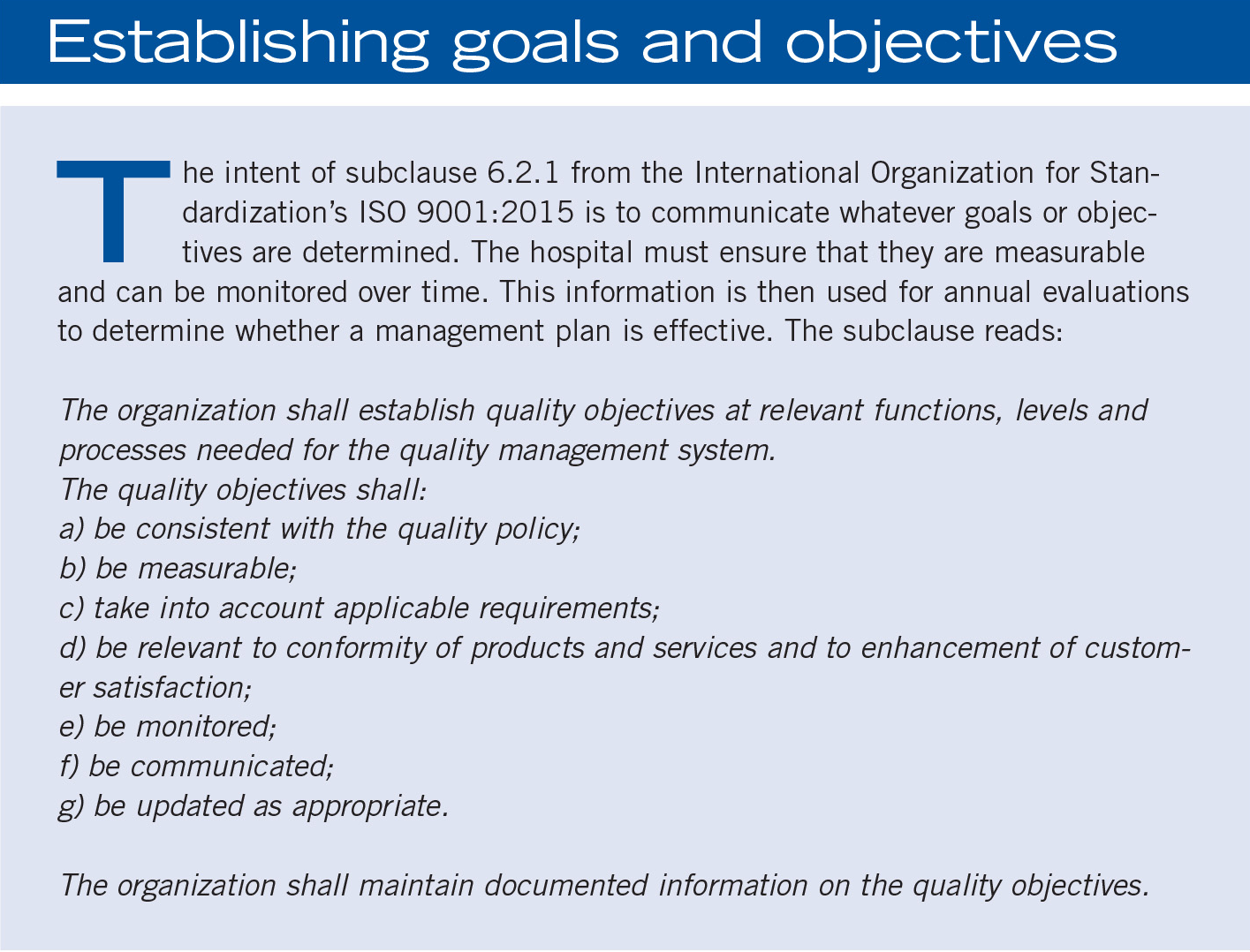
The International Organization for Standardization’s ISO 9001:2015 Quality management systems — Requirements and CMS allow a wide range of possibilities when it comes to how an organization determines competence and qualifications for staff in a hospital to meet the CoPs.
This is true not only for clinical staff, but also the physical environment. Consider the following: how many hospitals have developed and maintained formalized processes to ensure that properly qualified individuals are maintaining critical infrastructure equipment like the emergency generator, chiller or the cooling tower?
While most facilities recruit and hire staff with experience and knowledge in these areas, many opportunities are lost by not validating the background and experience of all facilities and engineering staff. Hospitals do it with nurses and doctors all the time before they are allowed to interact with patients, why not facilities and engineering as well?
Take, for example, a large organization with multiple free-standing structures, each with their own differing patient care population, dedicated facilities staff and their own emergency generators. How does the organization ensure that all emergency generators are being properly maintained in a similar fashion by each individual staff member in a consistent and effective way?
A similar concept can apply within a small organization. For example, two engineers work together and cover for each other when the other takes time off. How does the hospital ensure each staff member is properly maintaining the equipment? While this is left up to the organization, the effect of an adverse outcome would impact the patient population.
Core concepts
Regardless of the area of the physical environment that is under consideration, the core concepts of combining planning, preparation, resource allocation, corrective action(s) and evaluations for effectiveness allow hospitals to determine what works, what doesn’t work and what needs to change to ultimately achieve continual improvement.
To reinforce the theme of risk-based thinking, facilities professionals should understand who they are and what they do, determine what can be done internally and what needs to be contracted out and, finally, be willing to step out of their comfort zones.
This will allow health care facilities professionals to challenge themselves and others to manage the physical environment not based on the way others think it should be done, but due to the various forms of risk that are present and unique to an individual organization.
A small acute care hospital in the South had a tight budget and a limited facilities management department of 2.5 full-time equivalent (FTE) employees. Over the course of three months, the facilities director went on a medical leave of absence, the assistant facilities director left to go to another organization a month later, and the remaining half FTE was limited in availability due to other commitments outside the organization.
During the recruiting process to replace the assistant facilities director and awaiting the return of the facilities director, the administration of the hospital decided to shift responsibility of oversight of the physical environment to the director of human resources until the facilities director returned. The thinking went: It’s only going to be about a month or so, what could possibly happen?
Close to midnight on a Friday, the hospital was subjected to the direct impact of a lightning strike. Thankfully, and most importantly, there were no injuries or significant structural damage to the building. However, the lightning strike shorted out and completely fried the only fire alarm panel in the building.
The lightning strike was not loud or significant enough to draw the attention of the limited staff in the building at the time. Early the next morning, the local fire marshal arrived as he was notified by the fire department of the loss of communication between the hospital and the fire department. The fire alarm panel was quickly identified as inoperable and subsequently red tagged for an immediate repair needed.
The fire marshal left a written report with the charge nurse on-site, who then put the notice in the mailbox of the facilities director, who was still on medical leave. However, the charge nurse was unaware of this and did not know the director of human resources was in charge during the interim. Three days later, a survey team arrived on-site. The physical environment and life safety surveyor identified the fire alarm panel as inoperable and red tagged by the local fire marshal.
When the surveyor shared this information with the administration and “interim” director of facilities for the hospital, they were unaware of the current condition and did not have a plan in place to protect the patients, staff, visitors and overall health care environment from a potential fire over the previous four days.
This story introduces several questions that hospital facilities professionals must consider in their operations. They include:
- If a key position is open, how does the hospital reassign high-risk roles and responsibilities?
- How does the hospital communicate key internal changes related to high-risk areas or processes?
- What are the competencies, authorities and awareness of the on-call administrator?
- What type of plans are necessary from a capital expenditure program for emergency repairs?
- Given certain conditions, how, why, when and where do patients need to be evacuated?
About this article
This article is a joint project of Health Facilities Management magazine and DNV Healthcare USA Inc.
Brennan P. Scott, CHOP, CHFM, is program manager for acute care/critical access hospital services, head of surveyor development and educator/trainer for DNV Healthcare USA Inc. He can be reached at brennan.p.scott@dnv.com.
Related Articles
Preventing a possible outbreak through emergency response and remediation
Lessons learned from a real-life hospital flooding scenario and six steps for response.
Five things to include in a physical environment mitigation plan
A quick guide on how to identify and address physical environment issues quickly and effectively.

The facilities manager’s role in reducing healthcare-associated infections
From multidisciplinary communication to establishing safety procedures for construction, remediation and maintenance, facilities teams play a critical hand in reducing patient infections.