
A preview of changes to NFPA codes and standards

NFPA 99 addresses many integral systems, including medical gas, plumbing and electrical systems.
Left image courtesy of ASHE; center and right images by Getty Images
Health care facilities have been through a particularly challenging time these past few years. Overtaxed hospitals and seemingly endless supply chain issues have been at the forefront of everyone’s mind.
However, that does not mean that more typical concerns, like infection control and patient life safety, have disappeared. Fortunately, there are great resources for mitigating fire and life safety concerns.
The National Fire Protection Association’s NFPA 99, Health Care Facilities Code, and NFPA 101®, Life Safety Code®, have both been updated. Some changes are due to the COVID-19 pandemic, while others address sustainability concerns, and still others address new or emerging technologies.
Although the Centers for Medicare & Medicaid Services currently enforces the 2012 editions of these codes, a high-level look at some of the key changes in the 2024 editions can provide health care facilities professionals with ideas for process improvements and a glimpse of future regulatory changes.
NFPA 99 changes
NFPA 99, Health Care Facilities Code, contains a wide array of requirements that apply to health care facilities, addressing many of the integral systems that play a role in fire and life safety. These include medical gas systems, medical vacuum systems, electrical systems, information technology and communication systems, and plumbing and HVAC systems. Outside of those systems, NFPA 99 also addresses emergency management, security management, hyperbaric facilities, and electrical and gas equipment.
The 2024 edition of NFPA 99 introduces noteworthy changes that emphasize the evolving landscape of health care environments and the critical importance of maintaining top-tier safety levels for patients, staff and infrastructure. This edition’s major revisions make it a crucial update for health care professionals and facilities managers.
The COVID-19 pandemic stressed many health care facilities to their limits. It became evident that besides oxygen (which requires an emergency oxygen supply connection), many of the essential medical gas systems did not have the ability to easily connect to a supplementary supply. In the 2024 edition of NFPA 99, a new section has been added that requires all medical gas and vacuum systems to be provided with an auxiliary connection on the patient side of the source valve for connection to a temporary or supplemental source of supply.
Another consequence of the COVID-19 pandemic is that many facilities professionals are now worried about whether their medical gas and vacuum system piping is adequate to meet heightened demands, especially within individual zones. In response, the section on medical gas and vacuum pipe sizing and design has been updated. This requires a calculation to be performed to ensure that the pressure loss across the system doesn’t exceed 10% and that these calculations are retained as part of the facility’s permanent record.
In response to real-world incidents, new requirements for cryogenic liquid withdrawal and piping have been added to the 2024 edition. Cryogenic liquids are gases kept at temperatures so low they become liquid and are a common sight at modern health care facilities. These liquids present unique hazards associated with their extremely low temperatures and require specialized equipment and systems to ensure the safety of staff and patients.
For this reason, the 2024 edition of NFPA 99 has a new section dedicated to cryogenic liquid withdrawal as well as cryogenic liquid piping. It covers topics such as cryogenic liquid containers, the ventilation of spaces housing these containers, the materials used in these systems, pressure relief valves and manifold arrangements.
Another significant change for medical gas and vacuum systems installations is the addition of references to the ASSE International/International Association of Plumbing & Mechanical Officials/American National Standards Institute 6060, Professional Qualifications Standard for Medical Gas Systems Designers. The ASSE 6060 certification is for individuals who design new or existing medical gas systems. The certification covers the layout, sizing, and selection of equipment and piping, and the location of medical gas outlet/vacuum inlets.
As the world increasingly prioritizes environmental sustainability, the health care sector is likewise trying to reduce its environmental impact while maintaining fire and life safety levels. To ensure there are options for electrical backup power at varying levels of sustainability, much of the terminology around what was previously called alternate power sources has been changed.
The term “alternate power source” has been changed to power source. The term “emergency power supply,” often abbreviated as EPS, has been replaced with on-site power. In addition, many extracts and references to NFPA 110, Standard for Emergency and Standby Power Systems, have been removed from this edition to better allow the requirements to be applied to both generator and non-generator on-site power supplies.
As far as other significant electrical system updates go, some new paragraphs have been added to help consolidate the performance, testing and maintenance requirements into NFPA 99, and the ground-fault protection section has been restructured.
There have also been a lot of updates to the hyperbaric facilities chapter. Requirements around primary and secondary fire suppression systems for hyperbaric chambers have been added. Previously, there were only prescriptive requirements stating that a deluge-type water spray system and a handline needed to be installed in all Class A chambers. This language has been changed to include options for alternatives to both the deluge and handline systems.
The primary system can now either be a deluge system or some sort of alternative fire suppression approach with potentially different design features and suppression media. The caveat to the alternative fire suppression option is that it needs to meet specific testing criteria to demonstrate that the alternative approach will be effective. The secondary fire suppression system is permitted to either consist of handlines or portable fire extinguishers.
The 2024 edition of NFPA 99 is proof of the dynamic nature of health care facilities safety. By embracing changes brought to light by the COVID-19 pandemic, following and responding to real-world incidents and prioritizing environmental sustainability, this edition addresses the evolving needs of modern health care environments. As health care professionals and facilities managers navigate the complexities of patient care, they can turn to NFPA 99 as a comprehensive guide to ensure the highest standards of safety and compliance.
NFPA 101 revisions
One of the many challenges health care facilities faced in the wake of the COVID-19 pandemic was the overcrowding of hospitals. While it became apparent that temporary structures would be necessary to care for the influx of patients, it wasn’t clear how to erect these structures safely and quickly. Hotels were converted into health care facilities, temporary barracks were constructed to supplement the existing health care infrastructure and a variety of other solutions were used to provide the space necessary to treat patients.
While NFPA 101, Life Safety Code, has requirements for new health care occupancies as well as requirements for the change of occupancy of existing buildings, these requirements were not always feasible, given the time and cost restraints. As a result, the 2024 edition of NFPA 101 will contain requirements and a definition for alternative care sites (ACSs). These work together with a new annex to provide guidance and requirements that balance a minimum level of life safety with the urgent and temporary need for these types of facilities. The ACS annex provides considerations for the planning, design, construction, operation, maintenance and decommissioning of ACSs.
Another major change for health care occupancies is the expanded scope of the reference to NFPA 241, Standard for Safeguarding Construction, Alteration, and Demolition Operations. In prior editions of NFPA 101, for both new and existing health care occupancies, the means of egress in any area undergoing construction, repair or improvements needed to comply with NFPA 241. The 2024 edition of NFPA 101 now requires construction, repair and improvement operations to comply with NFPA 241. This means that NFPA 241 now needs to be looked at and implemented as a whole.
Health care occupancies conducting construction, repair or improvement operations will now be required to develop a fire prevention program (FPP). An FPP addresses several topics related to fire and life safety as well as emergency response, including pre-incident planning, site personnel responsibilities during an incident, procedures for reporting emergencies, evacuation procedures, site hot-work operations, fire protection systems, housekeeping, waste disposal and temporary utilities. Many of these topics may already be part of a facility’s pre-construction risk assessment.
NFPA 241 also requires the building owner to designate a FPP manager (FPPM) who is responsible for the FPP and carrying it out to its completion. The FPPM needs to be a competent person who has knowledge of applicable fire protection codes and standards, the fire protection systems available in the health care facility and fire inspection procedures. (This change was only made to new and existing health care occupancies; new and existing ambulatory health care occupancies still only require means of egress in any area undergoing construction, repair or improvements to comply with NFPA 241.)
The 2024 edition of NFPA 101 also contains a revision to the protection requirements for an increased maximum size for patient care sleeping suites. Previous editions permitted an increase in the maximum size of a patient care sleeping suite to 7,500 square feet (700 square meters) where the smoke compartment had additional protection. The 2024 edition allows for the same increase, but instead of the protection needing to be provided throughout the smoke compartment, it is only required to be provided throughout the suite.
Over the past several cycles, the Life Safety Code has expanded requirements for hazards beyond the traditional fire hazard, such as those associated with hazardous materials and carbon monoxide. Carbon monoxide detection is now required for new health care occupancies. Rooms containing permanently installed fuel-burning appliances, such as fireplaces, must have carbon monoxide detectors installed on the ceilings. Additionally, carbon monoxide detectors must be installed within 36 inches (910 millimeters) of the first supply air register from a permanently installed, fuel-burning HVAC system.
Sterile cores are now specifically identified as hazardous areas in both new and existing health care occupancies for the 2024 edition. The sterile cores must be protected by smoke partitions unless several criteria are met.
Another change associated with the protection of hazards in health care occupancies is related to the use of nonfunctioning, residential cooking equipment. When this cooking equipment is disconnected from power and fuel sources, and is used for rehabilitation, physical therapy or some other clinical purpose, the cooking equipment does not require additional protection.
Modular rooms and sleep pods have become increasingly popular, and the Life Safety Code now addresses these. These prefabricated rooms need to be listed, meet certain size restrictions and meet requirements related to interior finish. The installation location of modular rooms or sleep pods must also be evaluated. They must not obstruct the required means of egress for other areas in the building.
Particularly when installing sleep pods, the impact of providing sleeping accommodations in occupancies that may or may not have previously been used for sleeping needs to be carefully considered. Residential occupancies cannot be considered incidental and, therefore, the installation of sleeping accommodations can impact the occupancy classification of an existing space.
Based on feedback
As with every prior edition of NFPA 99 and NFPA 101, the 2024 editions were revised to improve minimum safety standards based on feedback from the field.
While this edition cycle is unique in that there were several changes related to lessons learned from operating during a global pandemic, there are also many changes related to emerging technology, sustainability concerns and common industry trends.
This article only highlights a few key changes related to health care facilities. For a complete view of changes, the NFPA 99 and NFPA 101 first and second draft reports are available for review online.
Getting involved in the NFPA codes development process
Health care facilities professionals who face code compliance challenges they think are impractical can help to change them. That’s because the public is encouraged to participate in the National Fire Protection Association (NFPA) codes and standards process.
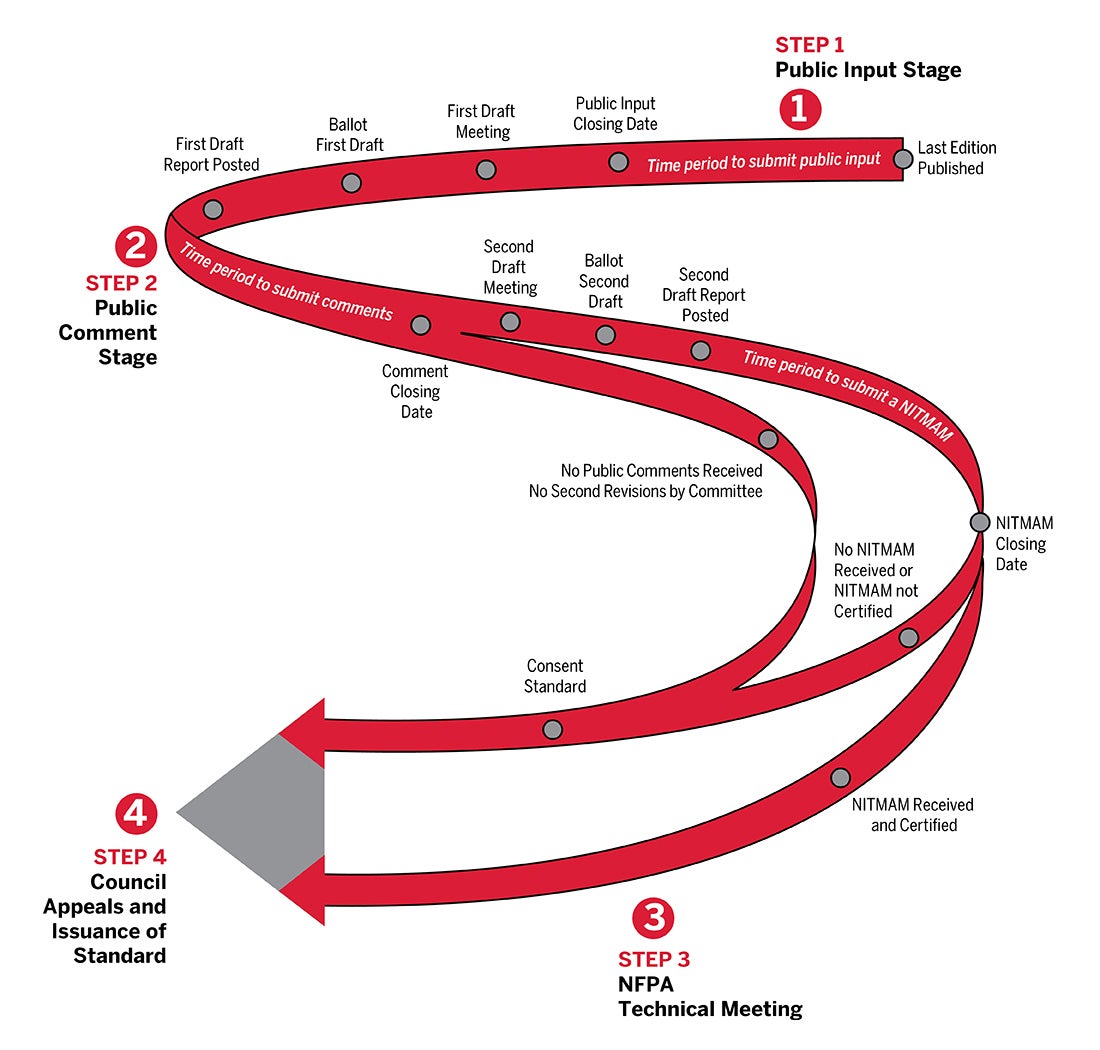
After a new edition is released, a document will open for public input. This is the public’s opportunity to propose changes. To submit public input, facilities professionals should go to "nfpa.org/doc#" (e.g., for NFPA 101, go to nfpa.org/101). Once there, they can select the “Next Edition” tab and click the link “The next edition is now open for input.” They will need to sign in or create a free account. Then, they can submit any changes they want the technical committee to consider. It is always a good idea to provide technical justification for why the change should be made.
Once the public input stage is closed, the technical committee will hold its first draft meeting. All public inputs are reviewed and responded to during this meeting. Any proposed changes will be voted on via a letter ballot before they become part of the document. Once the letter ballots have been received, a first draft report is posted.
The document then opens for public comment. Again, the public can propose changes. Once the public comment period is closed, the committee holds a second draft meeting to discuss changes and respond to all public comments.
During the second draft meeting, changes can only be made to topics addressed during the first draft meeting. This means either a change needed to be made or a public input needed to be submitted during the first draft stage. Both the first and second draft meetings are open to the public, but the technical committee chair decides if guests are permitted to speak. A more detailed description of the NFPA process is available online.
If facilities professionals are looking for a more substantial way to participate, they can apply to be on a technical committee. To do so, they should visit the document information page and select the “technical committee” tab. Under “committee membership” will be a link to “apply to committee.” This will take facilities professionals to an online application that will be reviewed for appointment. More information on becoming a technical committee member can be found on NFPA's website.
Val Ziavras, PE, is technical services senior engineer, and Brian O’Connor, PE, is technical services engineer at the National Fire Protection Association. They can be contacted at vziavras@nfpa.org and boconnor@nfpa.org.
Related Articles

CMS data highlights opportunities to advance emergency preparedness
Here are the five most commonly cited emergency preparedness deficiencies at hospitals and tips on how to correct them.

The EVS professional's role in managing old and new pathogens
What environmental services departments should know about pathogens like measles and bird flu and how to stop their spread.

ASHE launches committee to help answer member questions
The new MyASHE Response Committee will work in coordination with the ASHE Regulatory Affairs Team to monitor and respond to critical questions.