
Build a ‘see something, say something’ safety culture
Clinical and nonclinical staff should all be on the lookout for safety concerns and be familiar with environment of care protocols.
Image from Getty Images
Creating a safe environment is a core duty in every health care organization, and it does not happen by accident. It takes careful planning, strong teamwork and a culture that puts safety first.
A strong safety culture requires commitment from leaders and staff at every level. Executive leaders, managers and front-line employees must support an environment where safety is respected, discussed and improved over time. This culture grows with communication, accountability and visible, supportive leadership. When leaders listen to concerns and follow up, employees see that safety matters. In turn, staff who feel heard speak up early and help solve problems. Creating this psychological safety for front-line employees is vitally important since they are often the ones to notice risks first.
Taking a holistic approach to safety
To manage safety well, facilities leaders must look at the entire physical environment. Each location or occupancy type will affect safety, and every department has a role. Many departments share overlapping responsibilities, including environmental health and safety, maintenance, patient safety, quality, infection prevention and control, nursing, security, environmental services, projects and construction teams, and patient ambassadors or greeters. Each group brings a unique perspective and can spot unique risks. When these teams work together, they create a strong safety net for staff, patients and visitors.
“See something, say something” should be encouraged, as no one should walk past a concern or assume someone else will report it. For example, a dietary employee leaving work notices the back exit door is not closing and locking properly. The hope is that person knows how to report it to security and feels safe to do so. A healthy culture shows in daily actions and shared responsibility.
Facilities leaders, safety managers and environmental health professionals can access tools, resources and best practices (some of which are shared in this article) to build strong safety programs where a “see something, say something” culture can flourish. Used well, these tools help staff spot hazards early, communicate clearly and fix problems quickly. A safe facility starts with leadership, but it reflects in employees working together daily, following clear procedures and protecting everyone who enters the building.
Leveraging existing safety tools
A practical way to review the physical environment is to divide facilities into key sections, such as public areas, support zones, patient care floors, perioperative areas and mechanical rooms. Each area carries its own unique risks, so safety rounds should be tailored to the specific needs of each space.
Accurate documentation is essential for this to work effectively. Facilities staff should use paper forms, online tools or digital rounding platforms to record their observations and share findings with the appropriate teams. Any issues identified should be corrected promptly, tracked through work orders and followed through until completion to ensure the loop is fully closed. When a hazard is found, a safety risk assessment should be completed to mitigate the risk and correct any deficiency right away. This process builds trust and shows that staff input leads to real, meaningful improvements.
The American Society for Health Care Engineering (ASHE) Resource Library provides many valuable resources, including sample documents, such as the Fire Safety Evaluation System for Healthcare Occupancies Tool and the Hazardous Vulnerability Assessment Tool). Another resource, the NFPA 99-2021 Risk Assessment Tool, can be referenced to help evaluate and align the clinical needs of a particular space. Many of the tools have been created with the input of ASHE members and are free to fellow members.
These templates, checklists and guides are useful for both new and established programs. Facilities can develop a tool matrix that lists which forms and resources each department needs. This helps standardize processes and is especially useful for onboarding new employees. As buildings grow, undergo renovation or change operations, the matrix should be reviewed and updated regularly to ensure it remains accurate and effective.
Hospitals also should make sure that safety committees and multidisciplinary teams report to the organization’s environment of care committee, often called the physical environment care committee. This structure helps leaders review all safety work in one place. In many systems, the committee also reports to the organization’s medical board so important issues receive proper attention.
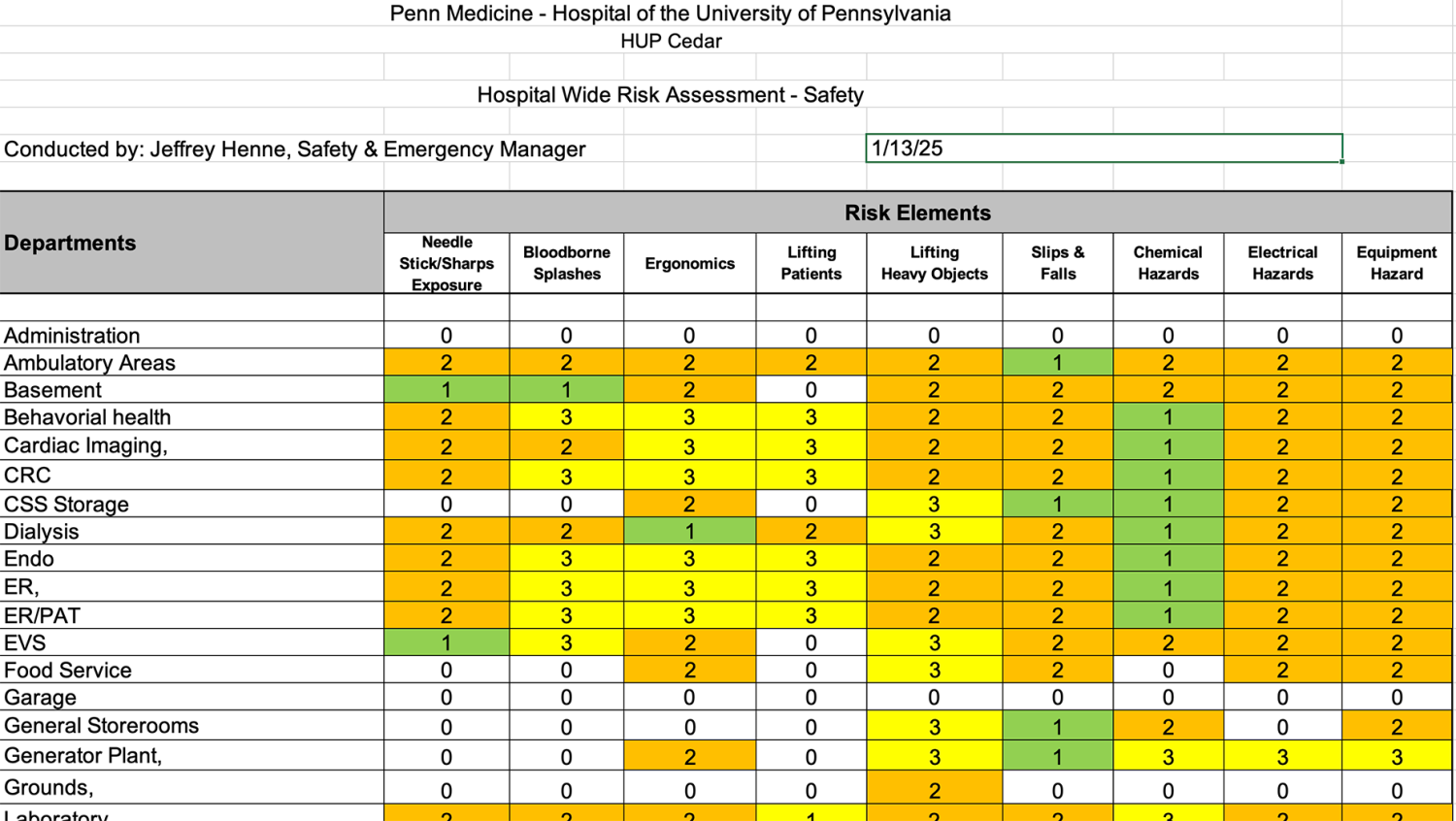
Click image to expand
In all main common areas and front entrance locations, it is important for the facility to complete at least an annual inspection, unless a regular schedule is already in place. During these inspections, staff should check the condition of all furniture used by visitors, family members and employees every day. They should look for worn or torn materials, faded colors or any other visible damage. Staff also should check for trip hazards, broken floor tiles, issues in elevator lobbies and faded or incorrect signage. Any personal items found should be collected and turned in to the security department for lost and found.
Finally, regular risk assessments are essential for compliance and prevention, such as ensuring oxygen tanks are stored safely. ASHE provides tools for Life Safety Risk assessments, and the Occupational Safety and Health Administration offers the Job Hazard Analysis Worksheet to outline job‑specific risks and controls. Used together, these resources support a proactive approach to identifying hazards, training staff and creating a safer environment for everyone. The example above shows an example of how these tools can be modified for a facility.
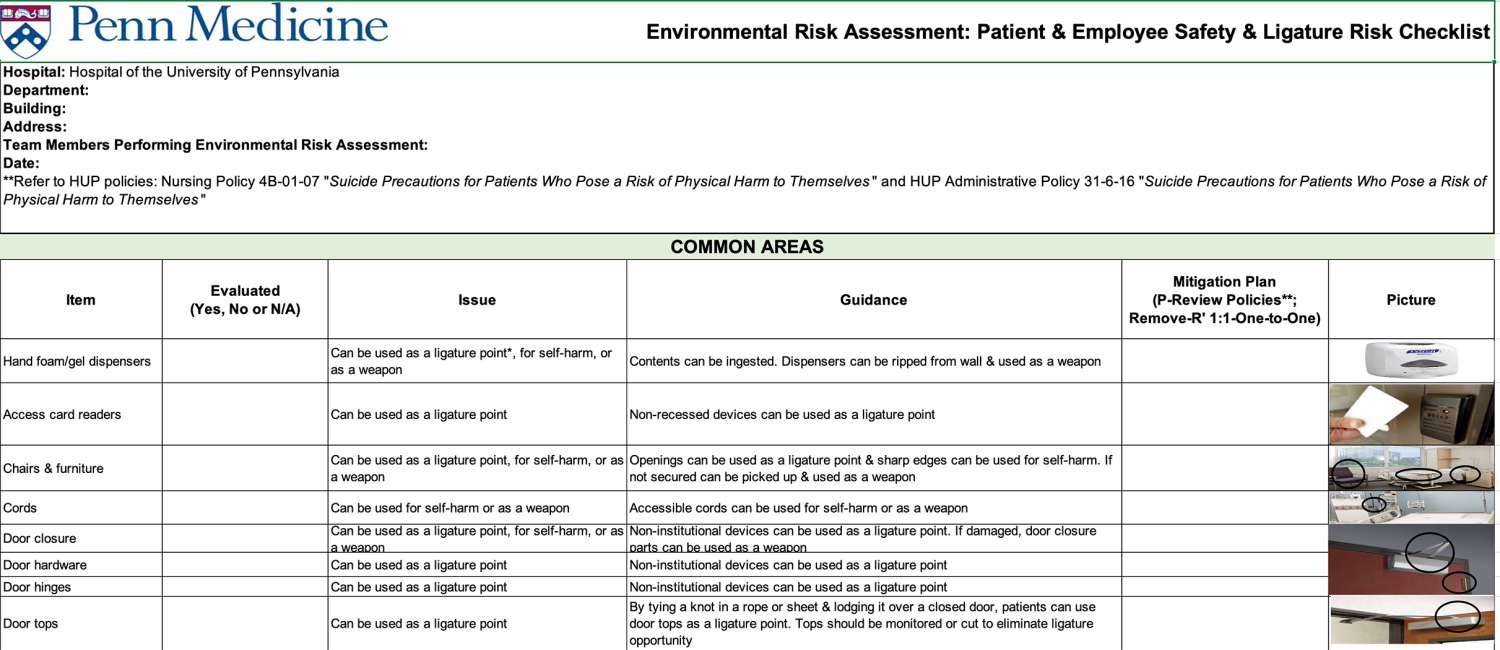
Click image to expand
Another helpful resource for engaging staff is the Patient Safety and Ligature Identification Checklist: For Ligature Resistant Common Items tool developed by ASHE (see left). This tool is designed to review all areas of a patient unit, including behavioral health spaces and common areas. It can be used during staff meetings or huddles to walk through each area, document what is found and support annual training.
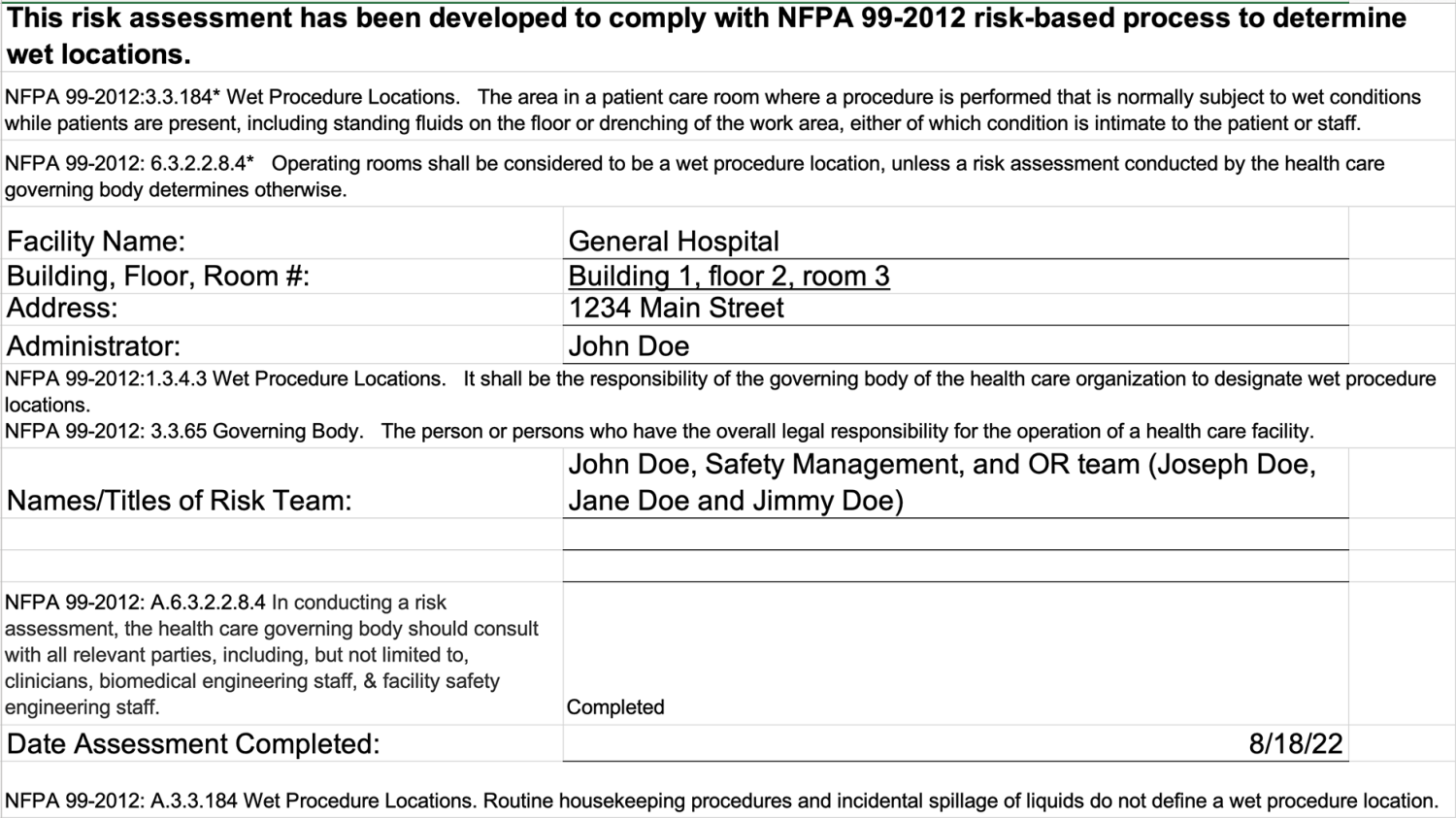
Click image to expand
An example for risk assessment of perioperative support areas is when a multidisciplinary team completes an annual review of wet‑location risk assessments. This review helps them work with perioperative partners to identify and confirm which operating rooms and procedural spaces should be classified as wet locations. An example of the NFPA 99-2021 Risk Assessment Tool used for this process is shown to the right. It is helpful for a small committee to meet, review the tool together and walk through each part as a team.
Safety considerations across departments
Security departments also play a key role in safety. Many hospitals have a workplace violence committee that reviews high‑risk areas and shares facility security risk assessments with the physical environment care committee. Women’s health departments often maintain an infant abduction committee to support Code Amber and infant‑abduction drills in hospitals.
A helpful technology for security departments is a touchless screening system that detects weapons quickly. These systems can screen many people at once, reducing long lines and delays at hospital entrances and in some cases allowing hospitals to forgo handheld metal detector screening. Weapons detection systems check for firearms, knives, clubs, explosive devices, pepper spray, shanks and other dangerous items. If a weapon or dangerous item is detected, security teams must insist that the item be surrendered or taken home.
Another key part of safety inspections is reviewing the location and condition of the facility’s automated external defibrillators (AEDs). Staff should confirm who completed the most recent inspection for each unit and make sure it followed the manufacturer’s recommendations. The AED battery, pads and unit must all be intact and ready to use. The biomedical department should complete an annual review to update the software, pads and batteries as needed. It is also helpful for certain departments to receive training on how to use an AED, especially since most models are designed to be simple and user‑friendly.
Another good practice that will aid first responders in their work is to place Stop the Bleed kits near the AED cabinets. These bright orange backpack‑style kits are designed to help responders during a mass‑casualty or active‑shooter event. While some items inside the kits have expiration dates, they do not contain any medications, so temperature and humidity are not a concern. It is important for the facility to follow a regular inspection schedule to make sure each kit is intact, fully stocked and ready to use.
There also are many other types of safety inspections a facility should consider. These include hand‑hygiene rounds, stair tower inspections, exterior ground rounds, rooftop safety checks, confined space reviews, fire department connection inspections, kitchen hood inspections, mechanical room safety reviews and laboratory inspections.
Teamwork and commitment
Using inspection tools and safety resources such as those shared in this article will help to consistently document findings in all common areas so that facilities can track problems and spot trends that need correction.
Building a strong safety culture takes time and requires commitment and teamwork from every department. When everyone works together, facilities become safer for staff, patients and visitors.
Tools shared in this article
All the tools and resources shared in this article are linked below.
- Fire Safety Evaluation System for Healthcare Occupancies Tool
- Hazard Vulnerability Assessment Tool
- NFPA 99 2021 Risk Assessment Tool
- Life Safety Risk Assessment Tool
- Identifying Hazard Control Options: Job Hazard Analysis
- Patient Safety Tools and Resources: Preventing Self Harm and Ligature Risks
Back to Member to Member series
Jeffrey E. Henne, CHC, CHSP, CHEP, CHFSM, CHPCP, FASHE, director of safety – Philadelphia operations and safety, emergency management and business continuity, Hospital of the University of Pennsylvania, and Khuong Huynh, MSITM, BSEE, CHFM, CHC, SASHE, assistant vice president of facilities, Penn Presbyterian Medical Center.
Related Articles

Being a good steward of health care finances
Learning budgeting basics and adopting the right financial language will ensure facilities departments are aligned with their organization's overall mission.

Training the next generation of facilities managers
Developing a site-specific training framework by combining institutional knowledge with industrywide best practices.

Prioritizing the health of operational assets
Strategies to move away from the break-fix model and adopt proactive asset management instead.