
The results of chlorine dioxide use after 23 years — Part 2
Editor’s note: This article is a continuation of “The results of chlorine dioxide use after 23 years – Part 1” article, which detailed the background, system design and initial implementation of a chlorine dioxide disinfection system at Johns Hopkins Hospital.
The Johns Hopkins Hospital in Baltimore has been using chlorine dioxide (ClO2) treatment systems since 2001 to mitigate the presence of Legionella in its inpatient buildings. After more than two decades of extensive testing conducted in four buildings, the health system is sharing the results of its program.
Chlorine dioxide (ClO2) system operation. The potable water flow control system for each (ClO2) unit consists of a flow meter, ClO2residual monitors and a computer control system. The flow meter monitors water use, and the computer control system collects flow meter data. ClO2 is injected into the potable cold water and hot water systems through injection quills. The ClO2 residual monitor controls the injection pump(s) to maintain ClO2 residual setpoints. The ClO2 residual monitor shuts down the ClO2 injection pump if necessary, so as not to exceed the Environmental Protection Agency’s (EPA’s) Maximum Residual Disinfectant Levels (MRDL) of 0.8 milligrams per liter of ClO2. The ClO2 controller and probe are calibrated weekly. The ClO2 monitor controlling the ClO2 residual has proven to be very effective.
ClO2 and chlorite levels. The overall operation and control of the ClO2 generators were found to be safe based on continuous ClO2 residual testing of the water in accordance with EPA regulations for ClO2.
The hospital residual testing data and Legionella water culturing data identified that the most effective chemical level of ClO2 is 0.5 milligrams per liter at the injection point in the potable cold and hot water piping mains to have detectable chemical residual levels at the end of the water systems. The level of ClO2 and ClO-negative 2 residuals throughout the buildings (distal sites) were well below the EPA’s ClO2 MRDL and ClO-negative 2 Maximum Containment Level.
Impact on Legionella and biofilm. Legionella species are known to reside in biofilm inside of pipes and at flow-restrictive devices such as piping, faucets, aerators, showerheads, valves, etc.
The hospital’s test data indicates that ClO2 effectively penetrates and removes biofilm in the piping system and at flow-restrictive devices. The effectiveness was found to be diminished at distal taps that were used infrequently due to the loss of ClO2 residual. This issue was resolved by implementing daily flushing of sinks and showers in patient bathrooms as part of the hospital’s daily environmental cleaning procedures.
The impact on biofilm was based on ClO2 residuals, bacteria culture results, Legionella culture results and visual inspection of pipes. Biofilm can be clearly seen in Figure 1 (below), which shows a section of four-inch diameter copper hot water supply piping that was removed for inspection. Legionella and bacteria were detected in the biofilm. After implementing a ClO2 shock remediation/flush, the ClO2 treatment system was placed into operation. Following three weeks of daily exposure to 0.5 milligrams per liter of ClO2, another section of pipe was removed for inspection approximately 3 feet away from the first section of pipe. The treatment was successful in removing the biofilm as shown in Figure 2 (below). Swab samples obtained from the pipe were cultured for Legionella and bacteria, neither of which were detected.

From left: Figure 1 shows the presence of biofilm in a four-inch diameter copper pipe. Figure 2 shows the successful removal of biofilm following chlorine dioxide treatment.
Image courtesy of Gregory Bova
Corrosion and scale.Most of the hospital’s existing potable water main was galvanized piping. The piping and valves had corrosion, scale and debris buildup. The potable water main was replaced with stainless steel piping over a three-year period starting in 2019 and finishing in 2022.
In buildings that are being treated with ClO2, the water mains show no significant corrosion related to ClO2. The test data associated with the application of ClO2 appears to have no deleterious effects on the building’s piping.
However, pinhole leaks periodically occur in the building’s copper piping systems. Numerous pipe samples were sent to multiple laboratories for analysis. The laboratory reports identified the pinhole leaks were caused by either chlorine (Cl2), chloride (Cl), pipe flux or high water velocities. ClO2 has not been identified as cause of the pinhole leaks.
It was surmised that ClO2 removes the biofilm. This biofilm protects the piping from chlorine and chloride. Removal of the biofilm exposes the pipe to direct contact with residuals of chlorine and chloride, resulting in accelerated corrosion.
Options were evaluated, such as the injection of sodium silicate into the potable water distribution system to protect the piping material from chlorine and chloride. Minimal data exist related to the effectiveness of the addition of silica related to Cl2, Cl-negative and ClO2 treatment. Therefore, silica systems have not been installed at this time.
Remediation disinfection and ClO2 treatment system startup. The evaluation of commonly used methods to remediate potable water systems, such as hyperchlorination, monochloramine and super heating, were found ineffective methods for eliminating Legionella in a short period of time. The development and implementation of ClO2 as a shock remediation combined with a flush proved to be extremely effective against eliminating Legionella. This method, when applied as a startup of ClO2 systems in older buildings and new buildings before occupancy, was found to be very effective in the control and elimination of Legionella.
Legionella testing and monitoring. In 2001, Hopkins implemented an aggressive monitoring and control strategy that exceeded the common secondary disinfection practices used during that time. Today, Hopkins’ strategy is considered a hospital standard for current pathogen control treatment.
The hospital tests the water for Legionella using a zero-detection level goal. Testing is performed throughout the inpatient buildings. Samples are obtained quarterly and during and after water events, and when there is a possibly related clinical nosocomial Legionella in a patient. Samples are obtained to assess all inpatient care floors where plumbing fixtures are used both frequently and infrequently.
Water samples are also obtained from locations where potable water enters the buildings; at the potable water main after ClO2 treatment; at the hot water supply, which is downstream of the heating converters; at the hot water return; and at the distal sites at the end of each inpatient floor. For each water sample collected, direct and concentrated cultures are performed using a laboratory certified by the Centers for Disease Control and Prevention.
Water samples are obtained from the monitoring sites in 30 seconds at:
- Domestic potable water supply pre-treatment;
- Potable cold water supply post treatment;
- Potable cold water at the end of the system dedicated cold water faucet, such as a hose bib;
- Hot water supply; and
- Hot water return.
Water samples are also taken at first draw from inpatient sinks. Samples are taken from two patient rooms per inpatient floor at the end of the water system. Taking a first draw sample identifies the condition of each faucet since it shares both hot and cold water supply.
Timeline of Legionella testing
Appendix A – Building A (see below)
 Click image to expand
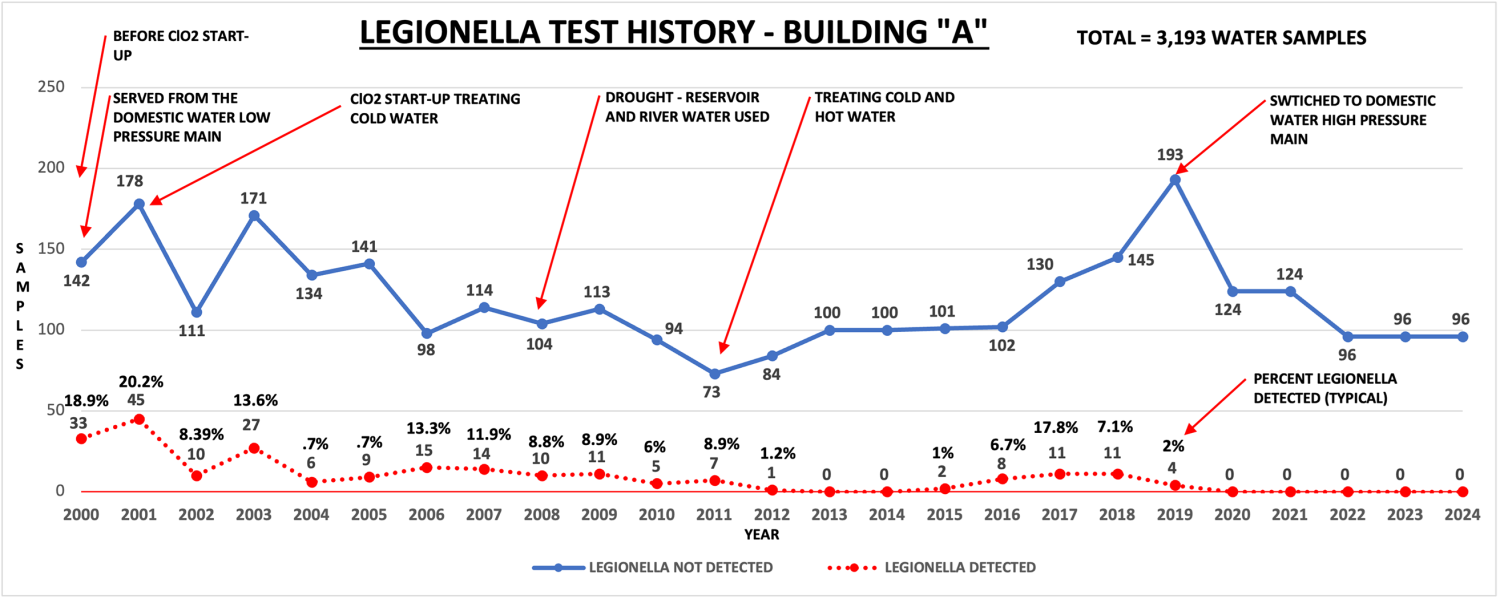
Click image to expandThis graph identifies the results found after 24 years of Legionella testing from 2000 to December 2024. It records 3,193 Legionella water samples obtained and 23 years of ClO2treatment. Below is a timeline of important findings:
- Between 2000 and 2019, the building was served from the city’s low-pressure potable water main.
- In 2000, before ClO2 treatment began, the building had a total of 18.9% Legionella detected at a maximum of 50 colony forming units (CFUs) of Legionella, with most samples at less than 10 CFUs of Legionella.
- In 2001, for the first year of ClO2 treatment, the building had a total of 20.2% Legionella detected at a maximum of 50 CFUs of Legionella, with most samples measuring less than 10 CFUs of Legionella.
- Between 2001 and 2011, the potable cold water system was treated with ClO2. The hot water system was not directly treated.
- Between 2002 and 2012, the building had a minimum of 0.7% to a maximum of 13.3% Legionella detected at a maximum of 500 CFUs of Legionella, with most samples measuring less than 10 CFUs of Legionella.
- Between 2011 and December 2024, in addition to the ClO2 treatment of the potable cold water system, the hot water system also was treated with ClO2. ClO2 was introduced into the hot water supply downstream of the converters.
- Between 2013 and 2014, the building had zero Legionella detected.
- Between 2015 and 2019, the building had 1% to 17.8% Legionella detected at a maximum of 390 CFU’s of Legionella, with most samples measuring less than 10 CFUs Legionella.
- In 2019, the hospital’s potable water main was replaced.
- In 2019, the building was switched from the city’s low-pressure potable water main to the city’s high-pressure potable water main.
- Between 2020 to December 2024, the building had zero Legionella detected.
Appendix B – Building B (see below)
 Click image to expand
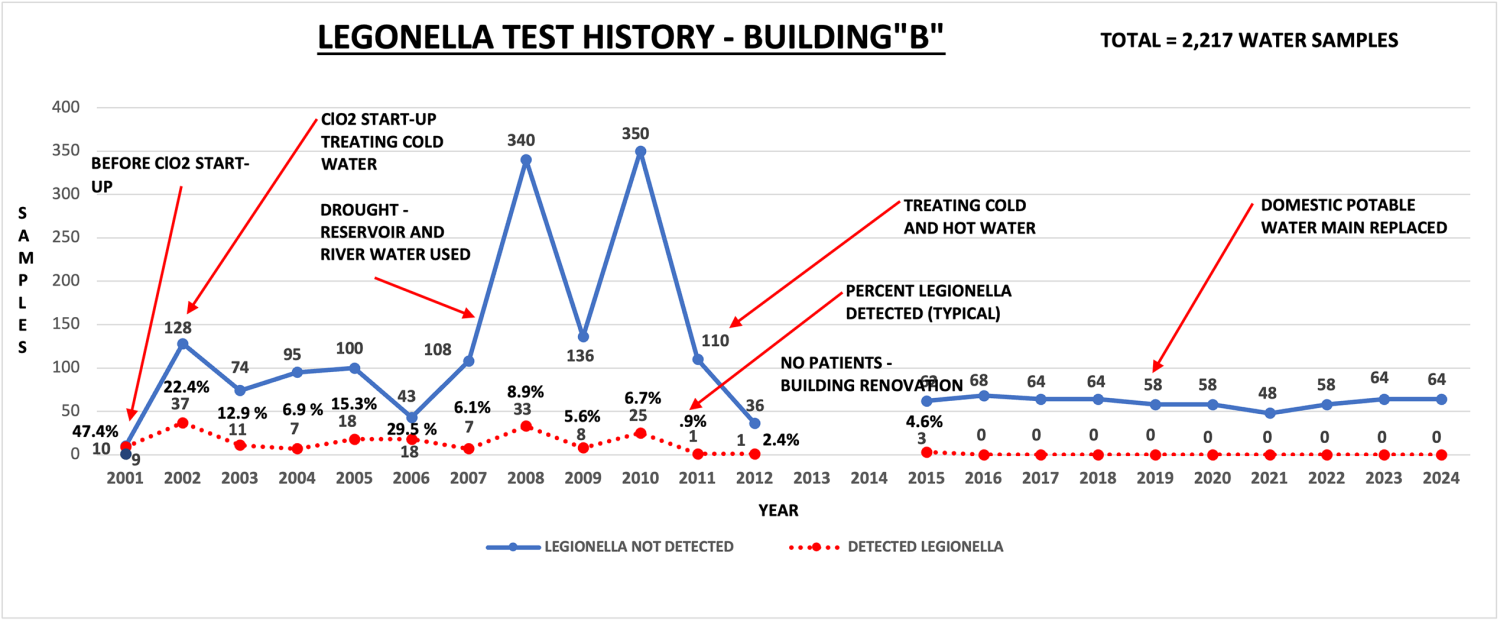
Click image to expandBuilding B is served by the city’s high-pressure potable water main. The graph below identifies 23 years of Legionella testing from 2001 to December 2024. It records 2,217 Legionella water samples obtained and 21 years of ClO2 treatment. Below is a timeline of important findings:
- In 2001, before ClO2 treatment, the building had a total of 47.4% Legionella detected at a maximum of 220 CFUs of Legionella, with most samples measuring greater than 50 CFUs of Legionella.
- Between 2002 and 2010, the potable cold water system was treated with ClO2. The hot water system was not directly treated.
- Between 2002 and 2011, after ClO2 treatment, the building had a minimum of 5.6% Legionella detected to a maximum of 29.5% at a maximum of less than 1,000 CFUs of Legionella, with most samples measuring less than 10 CFUs of Legionella.
- Between 2011 and December 2024, in addition to the ClO2 treatment of the potable cold water system, the hot water system was directly treated with ClO2. ClO2 was introduced in the hot water supply downstream of the converters.
- Between 2012 and 2014, Legionella testing was not done due to the building having no patients during the renovation of the patient wing.
- In 2015, there was a total of 4.6% Legionella detected. Three samples of Legionella were detected, with one sample at 260 CFUs of Legionella and the other samples at 20 CFUs of Legionella.
- In 2019, the hospital’s potable water main was replaced.
- Between 2016 and December 2024, the building had zero Legionella detected.
Appendix C – Building C (see below)
 Click image to expand
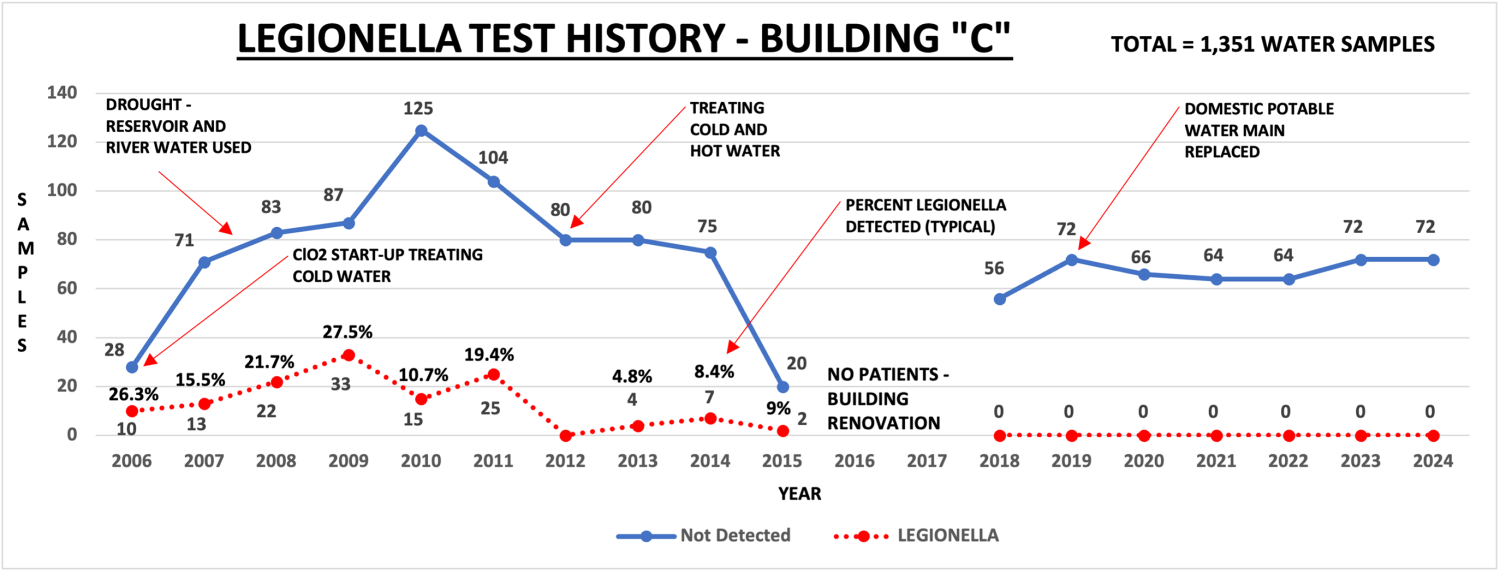
Click image to expandBuilding C is served by the city’s high-pressure potable water main. The graph below identifies 18 years of Legionella testing from 2006 to December 2024. It records 1,351 Legionella water samples obtained and 17 years of ClO2 treatment.
- Between 2006 and 2011, only the potable cold water was treated with ClO2. The hot water was not directly treated.
- Between 2006 and 2011, the building had a minimum of 15.5% to a maximum of 27.5% Legionella detected at a maximum of less than 3,000 CFUs of Legionella, with most samples under 50 CFUs of Legionella.
- Between 2012 and December 2024, in addition to the ClO2 treatment of the potable cold water system, the hot water system was treated with ClO2. ClO2 was introduced in the hot water supply downstream of the converters.
- In 2012, zero Legionella was detected.
- Between 2013 and 2015, the building had a total of 4.8% to a maximum of 9% Legionella detected at one to10 CFUs of Legionella.
- Between 2016 and 2017, Legionella testing was not done due to the building having no patients during renovation of the patient wing.
- In 2019, the hospital’s potable water main was replaced.
- Between 2018 and December 2024, the building had zero Legionella detected.
Appendix D – Building D (see below)
 Click image to expand
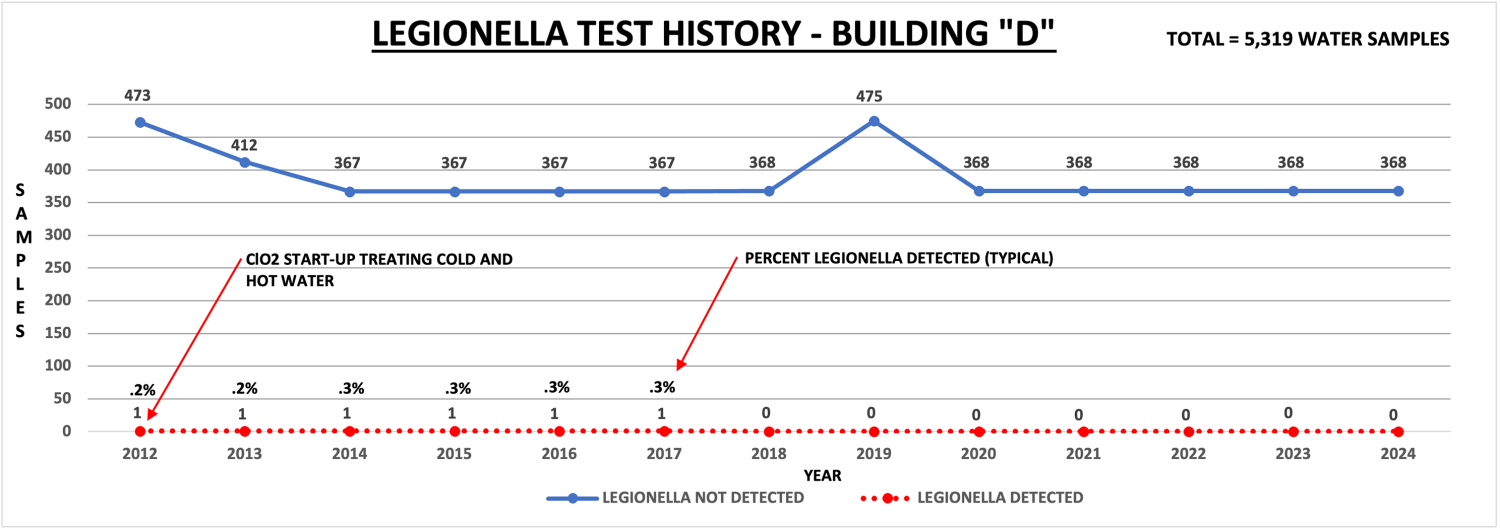
Click image to expandBuilding D is served by the city’s high-pressure potable water main. Both the potable cold and hot water systems are treated with ClO2. ClO2 treatment/flush was implemented before patient occupancy. Continuous ClO2 treatment was applied to the potable cold water system and hot water systems after treatment/flush.
The graph above identifies 12 years of Legionella testing from 2012 to December 2024. It records 5,319 Legionella water samples obtained and 12 years of ClO2 treatment.
- Between 2012 and 2017, the building had a maximum of 0.3% to a minimum of 0.2% Legionella detected at a maximum of less than 21 CFUs of Legionella at non-patient sinks. The non-patient sinks are not part of the patient room daily flushing.
- In 2019, the hospital’s potable water main was replaced.
- Between 2018 and December 2024, the building had zero Legionella detected.
Summary of findings
In the 23 years of using ClO2, there have been no nosocomial Legionella patients at Johns Hopkins Hospital. One patient tested positive for Legionella in Building B in 2008 and another tested positive in Building A in 2019. However, the patients’ Legionella serogroup could not be matched with water sampling. It was determined that the patients may have acquired Legionella before admittance.
The efficacy of ClO2 is influenced by proper treatment system design, operation, control and disinfectant residuals. Additionally, identifying and correcting piping deficiencies, application of equipment modifications to maximize their operation, installation of manual faucets, laminar flow control devices and understanding water usage are necessary to an effective Legionella prevention program. It is essential that daily flushing protocols and prompt remediation after disruptions to the potable water system be implemented.
After using ClO2 at Johns Hopkins Hospital for 23 years, extensive chemical testing and Legionella culture data affirms the safety and efficacy of ClO2 as a treatment strategy for removing biofilm, and controlling and eliminating Legionella.
Acknowledgments
The author of this paper would like to acknowledge and thank all those who were involved with this project over the past 23 years including:
- Anatoly Gimburg, vice president, facilities management, Johns Hopkins Health System.
- Lisa Maragakis, professor of medicine and epidemiology, Johns Hopkins University School of Medicine, and senior director, health care epidemiology and infection prevention, Johns Hopkins Health System.
Gregory Bova, Johns Hopkins Medicine, Baltimore.
Related Articles

Defining existing building commissioning
Health care facilities can use existing building commissioning to accomplish much more than just energy savings.
Preventing a possible outbreak through emergency response and remediation
Lessons learned from a real-life hospital flooding scenario and six steps for response.
Five things to include in a physical environment mitigation plan
A quick guide on how to identify and address physical environment issues quickly and effectively.