
Technologies to enable post-discharge communication
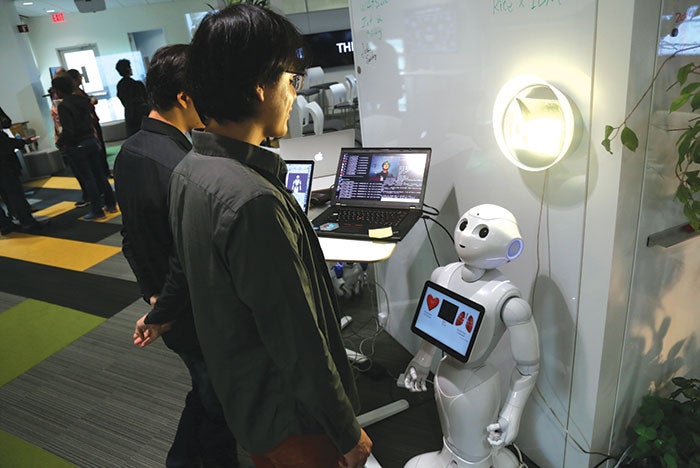
IBM’s Aging in Place think lab has developed a prototype robot called the multipurpose eldercare robot assistant.
According to the National Center for Health Statistics, more than 35 million hospital discharges occur annually in the United States. Most discharged patients go directly to their homes but, as of 2015, more than 8.3 million people received continued support from home health agencies, skilled nursing and long-term care facilities, hospices, residential care communities and adult day service centers.
With the goal of improving patient outcomes and reducing readmissions, many hospitals are focusing more attention on post-acute care, including long-term care (LTC) and skilled nursing facilities (SNFs). Some health systems have begun adding these facilities to their campuses, while others are creating networks of “preferred” facilities.
Among the systems that now partner with preferred SNFs are Advocate Health Care, the largest hospital network in Illinois; Banner Health in Arizona; the national Catholic Health Initiatives based in Colorado; the Cleveland Clinic; Henry Ford Health System based in Michigan; and Partners HealthCare in Massachusetts. Some health systems require SNFs to have electronic health record (EHR) systems.

Health care facilities are working to improve coordination of the continuum of care, but post-discharge communication to providers, patients and their families is extremely challenging.
For instance, millennials want instant mobile access to information; the sandwich generation adults, who care for aging parents while raising a family, need help juggling complex schedules; and baby boomers require diverse patient engagement techniques.
Combine these varied requirements with the need for data exchange between hospitals and post-acute care providers, and the result is a field that is being pushed for new post-discharge communication solutions. The effectiveness of these solutions will have a direct bearing on the quality of patient outcomes.
Impacting patient care
Once a patient leaves the hospital, communication gaps and fragmentation in the continuum of care arise all too easily.
You may also like |
| Technology and health facility design |
| Making technology talk beyond hospital walls |
| Medical grade wireless infrastructure |
|
|
Family support during post-acute care provides better outcomes, but paper care packets and patient portal information provided at discharge are often confusing to patients and family members. According to a report by Reuters, patients often feel disconnected with limited communication options — a problem that is exacerbated when an elderly patient is geographically separated from family members. Facilities that are moving into integrated patient and family engagement technologies have seen direct improvements in patient outcomes.
Many consumer-grade and enterprise-level technologies are available to support facilities’ post-care communication initiatives. These range from EHR interoperability to patient communication devices, medication adherence devices and remote patient monitoring. Each of these technologies requires clinician interaction, which will affect existing workflows and the built environment.
For instance, transfer of patient information to a SNF, LTC or home health organization may involve paper forms, including an EHR printout or a discharge plan that is typically 30 pages or more. While the EHR is now common in hospitals, post-acute facilities have not had the same incentives for implementation. In the past, many post-acute facilities were unable to justify the cost of EHR implementation, but industry drivers are changing that assessment.
With the increasing need for integration and exchange of information, EHR vendors are developing and introducing LTC products. For example, Kansas City, Mo.-based Cerner Corp.’s PowerChartLTC and CareTracker are specifically developed for the LTC and assisted-living market to integrate with its Millennium enterprise product. Epic Systems Corp., Verona, Wis., also is implementing a module for Partners HealthCare System to integrate its acute hospitals and Spaulding Rehabilitation Network of post-acute facilities.
Architects should consider the impact of these technology advances in facility design. Centralized post-discharge technology-monitoring spaces and work areas for collaboration of coordinated care are needed. Already overburdened information technology infrastructure and data centers will be further strained. Enhancing connectivity to other providers will become mission critical as interoperability and patient monitoring continue to expand beyond the walls of the hospital.

Mercy’s Virtual Care Center provides monitoring, consultations and telehealth for hospitals, primary care physicians and specialists.
Hospitals as hubs
Post-discharge monitoring, interactive patient and family engagement, and ongoing integrated data exchange between providers’ diverse platforms will drive hospitals to become the information hub for post-discharge care communication.
To coordinate the continuum of care between providers and patients, hospital operations centers (HOCs) are needed to address remote patient-monitoring devices. Staff will use population dashboards to track anomalies and identify potential adverse events that could trigger readmissions. Clinicians and technical specialists will monitor clinical alerts and reminders, prompting them to engage caregivers, patients and their families via video conference calls, emails and texts, and to dispatch mobile clinical teams.
Integrating clinical technologies into a centralized operations center will help clinicians to monitor key post-discharge patient risk factors, ranging from blood pressure changes to missed appointments, and improve clinical outcomes. The HOC will have telehealth pods for physicians and specialists to provide virtual post-discharge, follow-up visits to the patient’s home. To increase efficiencies, hospitals could combine the HOC with other systems that require ongoing monitoring of telemetry, security, fire alarm or bed management, creating a fully integrated, centralized command center.
Many health systems will have enough volume to warrant a virtual care center (VCC). The VCC will serve as a stand-alone facility, expanding the remote clinical technology abilities of the HOC to support such technologically advanced, integrated telehealth programs as eICU, telestroke and proactive case management of high-risk patients. The VCC also could connect to multiple HOCs and even serve as a modified medical office building of the future.
The natural progression of this approach to coordinated care also will create a need for wellness care centers (WCCs). WCCs will facilitate patient wellness programs that use technologies to engage patients interactively. Today’s accountable care organizations have laid the groundwork for these types of centers, and WCCs likely will expand quickly in this direction.

The patient attaches Preventice’s wireless patch to his or her body, which transmits biometric data to a phone and the cloud.
Pioneers in the virtual care arena that report cost savings and improved patient outcomes include:
Banner Health iCare. A combination of remote monitoring and telehealth, Banner Health’s iCare system uses analytics to detect adverse trends before they become larger problems. Patients check their blood pressure and weight daily and log that data into a custom tablet developed by Philips. The tablet also allows a patient to interact directly with his or her health team — primary care physician, pharmacist, nurse and health coach — to track and address any medical concerns.
Mercy Virtual Care Center. Mercy’s VCC in Missouri provides a range of services for bedside clinicians, primary providers and specialists — including telestroke, telesepsis and eICU as well as wellness, condition management and the Engagement@Home service. The combination of remote monitoring, remote consultations and analytics facilitates earlier diagnosis and intervention.
Other technologies
Beyond the hospital hub, many technologies on the market or under development can help health care systems to improve post-discharge communication and support coordinated care.
- Post-acute facility technologies. A few examples of technologies serving patients in the lower-cost post-acute setting include the following:
- Interactive TV solutions. San Diego-based Independa Inc.’s strategy is to consolidate fragmented technologies for medication management, socialization and remote monitoring, and situate their platform on a device every senior knows and understands: the television. The software provides video chat, photo sharing, messaging, local weather information and facility event information on a smart TV, navigated via the TV remote. Family members can communicate and track alerts from a dashboard that runs on a smartphone, tablet or computer. LG Electronics USA Inc., Englewood Cliffs, N.J., now embeds Independa software into its hospital and senior living TV models.
- Patient and staff tracking. Several systems configured and priced for the assisted-living or LTC market provide excellent location-based services for patient and staff tracking, wander prevention and nurse call. Traverse City, Mich.-based Versus Technology’s Visibility Resident Care system, for example, uses Wi-Fi, infrared and radio-frequency identification to track the location of patients and staff. As a result, LTC facilities can identify the staff member providing care to a resident, a wandering-risk patient straying into unapproved areas, and manage call response times.
- Stroke suits. Each year, 795,000 people in the U.S. suffer a stroke. The University of Twente in the Netherlands is developing a “stroke suit,” a wearable containing 41 sensors from the shoulders to booties on the feet. An internet-connected device transmits data to monitor and measure how patients actually move in the real world rather than how they move in a therapy session. The goal is to make rehab more efficient, saving treatment time and cost, and to help stroke patients regain the maximum level of movement and control.

Instead of a traditional pendant, UnaliWear’s smart alert device looks like a watch and can either respond to voice commands or unusual activity.
At-home technologies
As organizations increasingly seek to monitor patients in their homes, enabling technologies such as these are being introduced:
- Enhanced at-home monitoring. Sleep-therapy devices that monitor a patient’s cardiac rhythm accounted for 80 percent of all connected home-monitoring services in 2016. The monitoring applications include diagnosis (an alternative to the sleep lab), sleep therapy and streamlining of compliance monitoring for best outcomes.
- Mayo Clinic and Gentag Inc., Washington, D.C., are partnering to develop a disposable patch for diabetes management. This wearable device wirelessly sends information to the patient’s smartphone and is monitored remotely by the physician at the hospital or clinic.
- Alarm.com, based in Vienna, Va., uses intelligent sensors placed throughout the home to track and learn normal activity, such as how much time is spent in bed, in the kitchen or outside the home. When abnormal activity/inactivity occurs, notifications can be sent to the family member’s mobile device.
- At-home cardiac monitoring. Rochester, Minn.-based Preventice Technologies’ BodyGuardian Heart is a wireless wearable that securely sends biometric data to the patient’s smartphone and a cloud platform, using the phone’s cellular connection. The provider then accesses the data, which includes rhythm, atrial fibrillation, tachycardia, bradycardia, periodic electrocardiogram, average heart rate, respiration rate and activity level. Additional devices can remotely monitor blood pressure, weight, glucose and blood oxygen saturation levels.
- Voice-activated wearables. Seniors have been using medical alert pendants with voice communication since the 1980s. Some systems require a land line and are intended for use only inside the home, while others use global positioning systems and a smartphone or cellular connection to communicate with the monitoring center. All models require the wearer to push a button for assistance, which carries a stigma for some users.
- UnaliWear Inc., Austin, Texas, has developed a self-contained system that looks like a watch, uses cellular and Wi-Fi connections and operates by voice command. Monitoring staff also can initiate contact with the wearer for medication reminders and “Guide Me Home” assistance.
- Fall-risk mitigation devices. One in three Americans older than 65 will fall every year, and 75 percent of them will never regain their pre-fall mobility. Sensoria Inc., a Redmond, Wash.-based company with an established runners’ market for textile electronics socks, has developed a new app that evaluates fall risk in elderly patients or those recovering from injury, chronic conditions or stroke.
- ActiveProtective, Philadelphia, is developing a belt that senses when the wearer is falling and deploys an airbag in 60 milliseconds, protecting the person from the potential of a hip fracture. The belt also is equipped with Bluetooth technology that could send alerts to an emergency contact.
- University of Missouri’s Center for Eldercare & Rehabilitation Technology is trialing a technology utilizing cameras to detect falls in the home. Cameras extract patient silhouettes and combine with algorithms that send alerts when falls occur. Mission Health System of Asheville, N.C., is piloting similar technology: The Cerner Patient Observer monitors movement in multiple patient rooms from a central monitoring station. As these types of technologies advance, integrated, consumer-grade versions likely will provide greater opportunities in post-discharge communications.
- Robotic assistants. IBM’s “Aging in Place” think lab in Austin, Texas, has developed a prototype robot called the multipurpose eldercare robot assistant (MERA). The robot’s sensors initiate a call for help when they detect a variety of possible indicators of an emergency: unusual sounds or scents in the home; a stove that has been left on; when an older person has fallen; or sudden changes in the person’s heart rate or blood pressure.
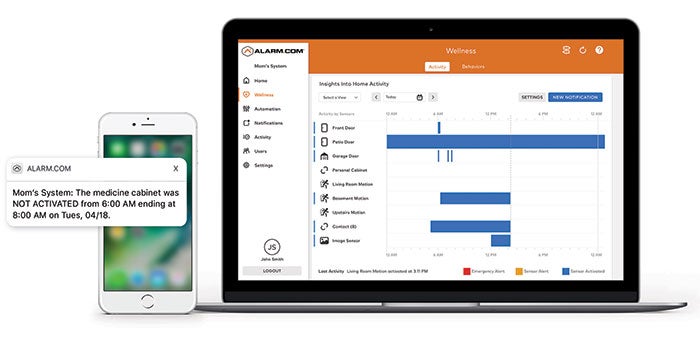
Alarm.com expands on fire and security monitoring with sensors placed throughout the home to track and learn normal activity and alert family members of problems.
Integrative imperative
Integrated clinical technologies are key to effective post-discharge communication and patient monitoring. To improve outcomes, avoid readmission costs and meet the evolving expectations of patients and their families, hospitals must become the communication hubs that facilitate true coordination of care.
Toward that end, hospitals must take the lead in facilitating the necessary monitoring and communication to provide a patient-centered, continuum of care, thinking “virtually” beyond the facility’s walls.
Ted Hood is principal and technology discipline leader and Jeff Looney is associate principal and technology team leader at Mazzetti+GBA, a global provider of health care mechanical-electrical-plumbing engineering design and technology/information technology consulting. They can be reached at thood@mazzetti.com and jlooney@mazzetti.com, respectively.
Related Articles

Health system invests millions in high-tech beds
NYC Health + Hospitals' upgrade marks a systemwide enhancement to patient comfort and care.

Agencies issue eight principles for OT cybersecurity
U.S. and international agencies released eight principles to eliminate cyber vulnerabilities in operational technology.

NFPA report reviews risks associated with smart buildings
The NFPA's Fire Protection Research Foundation report dissects the impact of smart building technology on life safety and presents a roadmap to address its challenges.