
Understanding recent door inspection and maintenance codes

Proper inspection and maintenance of fire doors is key to ensuring the reliability of life safety barriers.
Image courtesy of ASHE
Approximately one year after the implementation of Centers for Medicare & Medicaid Services (CMS) requirements for annual door inspections in health care facilities, an interesting phenomenon has developed.
More and more vendors are offering low- or no-cost inspections of fire and smoke doors to facilities, with the expectation that they will also be the vendor that completes the remediation and/or repairs. This has created large and sometimes inaccurate lists of deficiencies that may or may not be critical for repair.
It is imperative that facility managers understand the requirements of National Fire Protection Association’s NFPA 80, Standard for Fire Doors and Other Opening Protectives, and NFPA 105, Standard for Smoke Door Assemblies and Other Opening Protectives, before they approve repairs.
Alternatively, a third-party consultant or engineer may be used to evaluate the necessity and cost-effectiveness of the proposed repairs.
Full compliance
The Centers for Medicare and Medicaid Services (CMS) adopted the 2012 edition of NFPA 101, Life Safety Code®, effective July 5, 2016. NFPA 101 provides a fundamental basis for the inspection and certification of life safety services and features of health care occupancies by CMS.
NFPA 101 further adopts reference standards, including the 2010 editions of NFPA 80 and NFPA 105.
On July 28, 2017, CMS issued a memorandum that clarified requirements for the annual inspection and testing of certain door assemblies in health care occupancies in accordance with NFPA 80 and NFPA 105.
Full compliance with the inspection and testing requirements of NFPA 80 and NFPA 105 was required as of Jan. 1, 2018 (extended from the original compliance date of July 6, 2017, one year after the effective date of the 2012 Edition of NFPA 101).
Code basis
Paragraph 7.2.1.15 of the 2012 edition of NFPA 101 requires certain fire and smoke door assemblies to be inspected and tested annually in accordance with NFPA 80 and NFPA 105, where required by the occupancy-specific chapter. However, as the NFPA 101 health care occupancy chapters (i.e., chapters 18, 19, 20 and 21) do not directly reference paragraph 7.2.1.15, the annual inspection and testing requirements in that section do not apply to health care occupancies.
Further inspection of the NFPA 101 code requirements reveals that paragraph 8.3.3.1 requires that openings in fire resistance-rated assemblies (e.g., fire barriers) be protected by approved, listed and labeled fire door assemblies in accordance with NFPA 80, regardless of the occupancy. In addition, paragraph 4.6.12.1 further requires that any required feature be maintained in accordance with the applicable NFPA standards.
The proposed regulations were open to public comment as part of the adoption of the CMS Final Rule to amend the fire safety standards and adopt the 2012 edition of NFPA 101 for Medicare- and Medicaid-participating hospitals, critical access hospitals, long-term care facilities, intermediate care facilities for individuals with intellectual disabilities, ambulatory surgery centers, hospices that provide inpatient services, religious non-medical health care institutions, and programs of all-inclusive care for the elderly facilities.
More than 362 public comments were received concerning the proposed rule, including comments both in favor of and opposing requirements for annual inspection and maintenance of fire door assemblies. Commenters stated that the annual inspection of doors in an egress path is not required in health care, ambulatory care and business occupancies and that as hospitals are already performing visual inspection of fire door assemblies to ensure latching and smooth operations, an additional annual inspection would be unnecessarily burdensome on facility staff.
In response to the public comments and based on the above code references, CMS concluded that in health care occupancies, annual inspection and testing in accordance with NFPA 80 is required for all fire door assemblies and that documentation that the facility actually inspected and performed the necessary maintenance on these doors must be provided. Additional clarification was provided that the required annual inspection may be combined with maintenance efforts already in place at the facility.
CMS has further clarified that non-rated doors, including corridor doors to patient care rooms, are not subject to the annual inspection and testing requirements of either NFPA 80 or NFPA 105. However, good engineering practice requires that non-rated doors be routinely inspected as part of the facility maintenance program, as all required life safety features and systems must be maintained in proper working order.
Paragraph 5.2.4.2 of NFPA 80 outlines the following visual inspection criteria for swinging doors with builders or fire door hardware:
- No open holes or breaks exist in surfaces of either the door or frame.
- Glazing, vision light frames and glazing beads are intact and securely fastened in place, if so equipped.
- The door, frame, hinges, hardware and noncombustible threshold are secured, aligned and in working order with no visible signs of damage.
- No parts are missing or broken.
- Door clearances do not exceed three-quarters inch under the bottom of the door (as provided in Section 4.8.4) and one-eighth inch at the top, hinge and latch edges of the door (as provided in Section 6.3.1.7).
- The self-closing device is operational; that is, the active door completely closes when operated from the full open position.
- If a coordinator is installed, the inactive leaf closes before the active leaf.
- Latching hardware operates and secures the door when it is in the closed position.
- Auxiliary hardware items that interfere or prohibit operation are not installed on the door or frame.
- No field modifications to the door assembly have been performed that void the label.
- Gasketing and edge seals, where required, are inspected to verify their presence and integrity.
Similarly, paragraph 5.2.1 of NFPA 105 outlines the following visual inspection criteria for smoke doors:
- Doors shall be operated to confirm full closure.
- Hardware and gaskets shall be inspected, and any parts found to be damaged or inoperative shall be replaced.
Further requirements in NFPA 101 Section 8.5.4 limit the clearances for smoke barrier doors as provided above for fire-rated doors.
Qualified persons?
In 2017, ASHE published an article in response to questions raised by the inclusion of a requirement in the conditions of participation (CoP) from CMS for the annual inspection and maintenance of fire door assemblies by “qualified persons.”
NFPA 80 defines a qualified person as, “a person who, by possession of a recognized degree, certificate, professional standing, or skill, and who, by knowledge, training, and experience, has demonstrated the ability to deal with the subject matter, the work, or the project.”
While there are programs to qualify individuals as certified door inspectors, NFPA 101, NFPA 80 and NFPA 105 do not require that the inspections be performed by certified individuals. It is recognized that such certification programs offer a means by which to verify that the inspector is qualified but is not required by CMS or the accrediting organizations.
The article states that employees may be qualified by attending training through an official program or through on-the-job training, provided that the individual has “professional standing” or “skill” and either training or experience in fire and/or smoke door inspections.
For those facilities that want to use in-house personnel, there are training programs offered by several organizations, including ASHE and NFPA. Another effective approach is to have a qualified individual train in-house personnel in the facility using the fire and smoke doors that currently exist in the facility.
Given the volume of fire-rated doors, smoke doors and smoke barrier doors in any facility, many health facility professionals have chosen to outsource the annual inspection process to door vendors that are actively engaged in the sale, installation and repair of fire and smoke doors.
This has become a general practice, especially as some vendors are offering low- or no-cost inspections of fire and smoke doors to facilities with the expectation that they will also be the vendor that completes the remediation and/or repairs.
This has created large and sometimes inaccurate lists of deficiencies that may or may not be critical for repair. While this practice can include other systems and equipment for which inspection, testing and maintenance requirements exist, as a new requirement, it is becoming increasingly prevalent for door assemblies.
In many cases, the reports provided after an annual door inspection from such vendors can be overwhelming in the amount of information conveyed and unclear about which items are critical deficiencies and which are recommended actions.
In addition, vendors are not always versed in the applicable code requirements for existing versus new doors and specific requirements for special applications. Further, confusion may be added by the requirements of the adopted building code or fire code, which may differ from those of NFPA.
Careful review of the inspection report by a knowledgeable facility manager may assist in clarifying the deficiencies noted. Alternatively, third-party life safety experts and fire protection engineers can assist by examining the facility’s life safety program holistically, building from the foundation of the life safety plans to the implementation of the existing fire and smoke barriers and doors. The case studies accompanying this article illustrate the ongoing concern.
Additional research
ASHE has contracted with the Center for Health Design (CHD) to research why the failure rate of fire doors in hospitals is as high as is being documented during accreditation surveys.
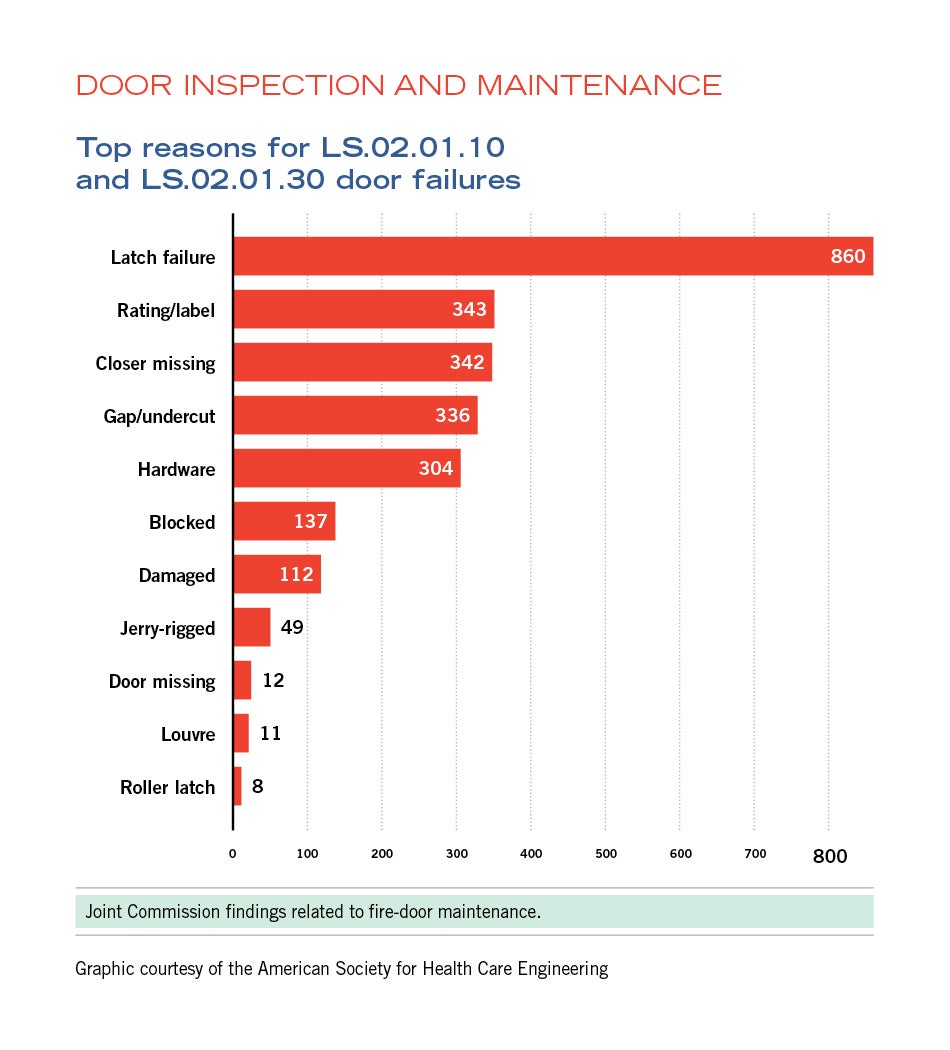
Joint Commission findings related to fire-door maintenance
Graphic courtesy of the ASHE
According to ASHE, the most common citations during accreditation surveys has been the failure of doors to properly latch. Doors that were working at the beginning of the survey fail during the surveyor’s test. The problem has existed for decades. During a recent “Focus on Compliance” project, it was discovered that over 30 percent of all door failure citations were due to a latch failure.
Thus far, the CHD research indicates that there may be other noncompliant conditions found during annual inspections that may be more prevalent than door latching failures. It is hoped that researching the cause of fire door failures may provide insight on how to resolve these issues and ensure the reliability of these life safety barriers.
The goal is for the research to be completed and a report presented at the 2019 ASHE Annual Conference & Technical Exhibition.
Cost-effective approach
Careful review of a vendor’s inspection report by a facility manager and/or review by a code consultant not involved in the repair or installation process may be a cost-effective way to parse inflated inspection reports to their root issues.
Third-party life safety experts and fire protection engineers can further assist by examining the facility’s life safety program holistically, further reducing the potential deficiencies and decreasing maintenance costs.
William Koffel, PE, FS-FPE, SASHE, is president, and Elizabeth C. Keller, PE, is fire protection engineer, with Koffel Associates Inc., Columbia, Md. William Koffel can be contacted at wkoffel@koffel.com.
Related Articles

Why portable weapons detection units should not be the default approach
Factors to consider when evaluating portable versus permanent weapons detection systems for healthcare facilities.

NFPA approves weapons detection amendment
Plus: CMS clarifies condition-level noncompliance oversight; ASHRAE introduces new energy-saving requirement; CISA releases guidance on zero trust adoption for OT.

CMS data highlights opportunities to advance emergency preparedness
Here are the five most commonly cited emergency preparedness deficiencies at hospitals and tips on how to correct them.