
Energy-saving ideas for every project

Photo by Getty Images
Hospitals are highly complex facilities, and many of the functions that take place within them consume a lot of energy. Together that combination creates a significant opportunity to reduce energy consumption.
A new American Society for Health Care Engineering (ASHE) monograph, “Reducing Operational Costs Through Energy Efficiency: Tips, Best Practices, and Case Studies from Energy Star® Hospitals,” describes many of these energy-saving opportunities.

The 80-page monograph was compiled by a variety of experts with diverse backgrounds from various geographical locations. Some of the tactics are common and have been explored before; some are less discussed and suggest additional options to consider.
Resources like the new monograph, which is excerpted for this article, are helping hospitals across the country work toward improved energy efficiency and greater savings.
Strategies for sustainability
There are several broad strategies hospitals and health systems can use to achieve greater energy efficiency, including the following measures covered in the ASHE monograph:
Benchmarking | Benchmarking a facility against its peers is the first step in a strong energy-management program. Through benchmarking, facilities can gain an understanding of how they are performing. Often, a hospital will benchmark to find itself to be performing in the lower tier of its peers. ASHE offers a free benchmarking and awards program called “Energy to Care” (www.energytocare.org), which imports data directly from the Environmental Protection Agency’s (EPA’s) Energy Star Portfolio Manager® and provides a dashboard tool so that managers can track energy use over time. Continually tracking energy has proven to be an essential component in managing a building’s energy.
Energy audits | An important best practice regarding energy savings is to conduct a periodic and thorough energy audit of a hospital. ASHRAE has designated three levels of audits to assess energy use: walk-through analysis, energy survey and analysis, and detailed analysis of capital-intensive modifications. A thorough audit includes a review of how the facility is consuming energy and how the facility procures the energy it consumes, and also examines both low-cost/no-cost opportunities and capital improvement measures in an effort to become more efficient.
Energy procurement | In many areas of the country, energy markets are partially or fully deregulated for electricity and/or natural gas. Deregulated markets tend to be more complex than regulated jurisdictions, but in many cases offer significant opportunities to save money through various procurement strategies. In regulated markets, facilities still can affect how their energy is procured. Utility rates, service standards and energy-efficiency programs often are regulated by a state commission. Most state commission websites provide information about ongoing dockets, regulations and rules. Facility professionals can participate with the commission through advocacy groups and public comment periods.
Recommissioning AND retrocommissioning | Recommissioning and retrocommissioning are two common approaches to comprehensive evaluation and implementation for performance improvements. Recommissioning is when a building seeks to test system operational performance to support energy efficiency and system reliability. A thorough recommissioning effort will bring the systems back to optimal performance levels and identify any needs to replace aging systems. If space uses and facility requirements have changed significantly from the original design, retrocommissioning may be more appropriate. Retrocommissioning starts by documenting current facility requirements (CFRs), which replace or amend the original owner’s project requirements used for commissioning. Then, the retrocommissioning team seeks opportunities to optimize the existing building systems to meet the CFRs.
Existing buildings
Existing health care facilities abound with opportunities to achieve greater energy savings, including the following measures, which are discussed in-depth in the ASHE monograph:
Control thermostats | Patients want control of the temperature of their rooms, as do clinical staff, so it's important to develop an internal standard that considers clinical needs. However, limiting the range of that control can save a lot of money without seriously affecting comfort. St. Anthony Hospital, Lakewood, Colo., saved $38,000 a year by limiting the patient control of thermostats. Patient rooms, operating rooms and central sterile processing usually are allowed slightly greater adjustability than the other 70 percent of a hospital’s square footage.
Additionally, variable air volume (VAV) systems are common in modern hospitals, and they save the most energy when the airflow is at the box minimum flow. By implementing an acceptable comfort range around the thermostat set temperature (known as a dead band), the time at minimum airflow is increased.
Finally, areas such as dining and waiting rooms, lobbies, lounges and corridors need to cater to many different users and thus should be set to a common setpoint (with dead band) that is acceptable to most people. Considering that corridors alone typically account for 25 percent of a hospital’s square footage, the impact of this change can be far-reaching.
Adjust variable air volume | While VAV boxes generally increase airflow with cooling demand, most designers traditionally set them to a fixed cubic feet per minute in heating to ensure that supply air doesn’t get too warm and stratify. As a result, as soon as a reheat valve cracks open to trim discharge air even slightly, the airflow may jump up to a higher heating value where it will remain for quite some time. Fortunately, most modern VAV controllers have built-in means to allow for heating airflow to increase only when heating demand is large. This is referred to as “dual-max VAV logic,” or letting the VAVs vary flow in heating.
Reduce airflows when code allows | Airflows are a key aspect to compliance in health care, and no one wants to install a system that might not have the capacity for tomorrow’s change in space use. Future capacity requirements can be established by the owner, equipment selected accordingly and systems set for the current condition’s lower requirements. However, any reductions to airflows in existing systems should be confirmed by an engineer and documented to show that air change and pressure requirements are maintained.
Optimize chillers | Many chillers run virtually continuously regardless of conditions. This doesn’t need to be the case; upgraded chillers run much more efficiently. For example, the Syracuse (N.Y.) VA Medical Center upgraded its chillers and added a system that optimizes efficiency based on current conditions. An algorithm takes data on temperature, humidity and other factors and calculates the most efficient temperature. A more dramatic upgrade took place at Advocate Illinois Masonic Medical Center in Chicago where the traditional primary/secondary chiller loop was replaced with a variable primary system. This system dispatches water as needed to meet the cooling load rather than continuously circulating water.
Use occupancy sensors | Some spaces are occupied inconsistently. Establishing a predetermined setback for a little-used meeting room is difficult if the room is occasionally used for unscheduled meetings. Occupancy sensors are one solution to that problem — the lights and ventilation come on automatically when the room is in use and turn off (or down) soon after the last person leaves. Occupancy sensors are commonly used in such areas as offices, storage rooms, toilet spaces, nurse stations, clean/soiled utility rooms, work spaces and break rooms. However, occupancy sensors are not recommended and are prohibited by the National Electric Code® in areas where an accidental turnoff will endanger an occupant. A cousin to the occupancy sensor is a heat sensor. St. Anthony Hospital put heat sensors in the kitchen range hood so that the fan would not run when not needed.
Conserve electricity | Round-the-clock operations and energy-intensive equipment cause hospitals to burn a lot of electricity, but hospitals have many opportunities to reduce electricity usage. In addition to setbacks, facility professionals may consider switching to light-emitting diodes (LEDs), which use less than half the wattage of fluorescent lamps and have a life expectancy of 50,000 to 100,000 hours. However, ballast and luminaire types must be taken into consideration. An LED retrofit kit will provide the best-quality lighting with the long life expectancy desired for LED energy and maintenance savings.
Utility rebates are often available for lighting retrofit projects. The energy savings must be documented during design and submitted to a third party for review. The rebate is often determined by the amount of energy savings associated with the project. Rebates help cover the cost of the project and lower the amount of time required for an owner to see a return on investment. Often these utility rebates will lock the facility into a specific utility cost. Every project should be evaluated individually to determine if the utility rebate is worth the change in utility rate.
Finally, the best way to save electricity is simply to turn off lights not being used. In addition to using setbacks and occupancy sensors, facility professionals can reduce unnecessary lighting usage by running campaigns that demonstrate how expensive lighting is.
Add heat-recovery elements | Heat-recovery elements can capture heat that goes out the smokestack or is otherwise lost to the outside. For example, many hospitals use heat exchangers or coils that extract heat, even small amounts, from air or water and loop it back into the hospital where it is used to heat the domestic hot water or the air entering the air handler. Those heat exchangers can be found in smokestacks, air handlers and even waste-water discharges.
Use variable-frequency drives (VFDs) | VFDs save energy in pumps and fans run by alternating-current motors. The VFD reduces the motor’s torque when full power is not needed. For example, without a VFD, the output from a pump is reduced by partially closing a valve, which doesn’t reduce the energy consumption of the pump; with a VFD, the speed of the pump motor is simply reduced as needed. Typically, VFDs work on three-phase induction motors, not on every motor.
Use fault-detection diagnostics (FDD) | All hospitals have some vintage of a building automation system (BAS) that controls the HVAC system. The BAS keeps systems running according to operating schedules, setpoints and fundamental sequences of operation. The programming coordinates the operation of thousands of components, including everything from boilers and chillers, air handlers and exhaust fans, dampers and valves. However, the programming in the BAS typically prioritizes the indoor environment (i.e., temperature, humidity or air changes per hour) over energy efficiency. Commissioning the system may have validated some sequences of operation from the design team to optimize energy use, but after operating for several months or years, system energy performance often drifts.
Continual retuning to maintain energy-efficient operations over time requires diligent monitoring at the BAS by a trained operator. Alternatively, FDD uses analytics software to continuously collect performance data from the BAS and identify potential faults. Faults are identified by evaluating a set of algorithms that are applied based on the system configuration.
While the BAS generates alarms, these alarms are typically simple notices that indicate a single sensor is reading outside of allowed setpoints. FDD algorithms are more sophisticated, capable of evaluating multiple variables to conclude that a fault may exist in the current operation. Once established, building systems are still controlled by the BAS, but the FDD service provides the operator with a real-time list of prioritized faults, visualization tools for analyzing trend data and a roll-up summary to track the status and resolution of identified faults.
Create a sustainability program and culture | As health systems are under continual pressure to reduce costs, the prospect of embracing efficient and sustainable operations has become increasingly popular. However, a health care organization needs to analyze its current state of sustainability before implementing any corrective measures. After completing a self-assessment and identifying potential areas of operational waste, facility professionals can develop a strategy to measure and track usage. Once a facility professional has assessed the facility’s needs and established a baseline of consumption and waste, he or she can create an interdepartmental team to help develop action plans and implement changes.
Work with the C-suite. C-suite support is essential to any initiative, sustainability included. The C-suite is always concerned about money, so being able to demonstrate the financial savings and avoided cost from energy-saving initiatives is important. Another way to develop strong support among the C-suite is to conduct regular VIP tours of the facility department.
Change the mindset of operations | Among other references, the Environmental Protection Agency’s 2014 guide, "Energy Star Treasure Hunt Guide: Simple Steps to Finding Energy Savings," provides a dynamic, effective process for identifying savings opportunities in existing equipment by optimizing resources and controlling operating costs. Recently, hospitals have begun piloting their own events. Participants include OSF HealthCare St. Joseph Medical Center in Bloomington, Ill. ($206,000 in energy savings); OSF HealthCare Holy Family Medical Center in Monmouth, Ill. ($89,500 in energy savings); and Atrium Health's Stanly Regional Medical Center in Albemarle, N.C. ($75,000 in energy savings).
New buildings
While energy-saving opportunities for retrofit applications are numerous, there are still more opportunities during the design and construction phases of a project, such as these from the ASHE monograph:
Achieve sustainability during building projects | The best times to initiate many sustainability initiatives are before and during construction projects. A project that is planned with sustainability in mind is naturally going to achieve better results than if sustainability projects are tacked on afterward. A new structure can be made more energy efficient in countless ways from the outset. A review of the LEED for Healthcare website (https://new.usgbc.org/leed) can provide scores of ideas.
It is also important to have the whole team on board early. A successful building project of any type, but especially one that includes unconventional energy-saving elements, creates a diverse, talented team that includes equal representation from owners, designers, construction and facility personnel. For example, when Methodist Olive Branch (Miss.) Hospital was planning its new building, which opened in 2013, the contractor, architect and engineer were all on a team that was motivated by the owners to create a highly efficient building. The effort paid off with LEED Gold for Healthcare certification.
During design and construction, sustainability concepts sometimes can add initial cost to a project, so it is important to show budget-concerned leaders the long-term payback for sustainability elements. For example, when Methodist Olive Branch Hospital considered installing a ground source heating/cooling system, the design team knew the initial cost would be higher than a conventional chiller/blower system. But the team quantified all the benefits, including lower construction costs resulting from the decreased need for ductwork and long-term energy savings, and convinced ownership that the system would quickly pay for itself.
Explore combined heat and power (CHP) | CHP systems, or cogeneration, provide an alternate source of electrical power and thermal heat than conventional utility generation. Electrical power is generated at the building site using an engine or turbine. CHP systems include production of both electric power and thermal heat energy for use on-site. These systems offer efficiency, economy, reliability and environmental benefits to hospital facilities compared with conventional electricity production at the utility power plant.
{kind=link}
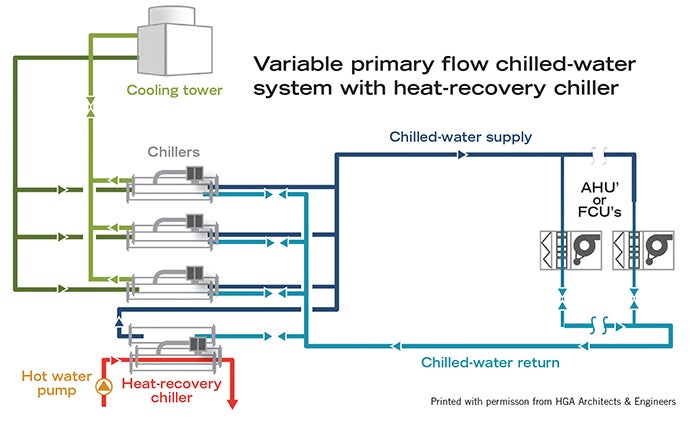
Consider heat-recovery chiller options | Demand for heating in a hospital can happen throughout the year, not just during periods of colder weather. Domestic hot water systems, building heat and process water heating represent a significant and consistent heating load in these facilities. In applications that require both chilled water for cooling and hot water for heating loads, a heat-recovery chiller can be used to capture and use heat that otherwise would be wasted to the environment.
Study boiler plant heat-recovery techniques | An enormous amount of cost and effort is associated with converting cold, raw water into chemically treated hot water/steam. Most health care facility professionals understand the basics of how boiler plants produce and distribute hot water/steam to meet the demand of various loads throughout hospital campuses. However, it is equally important to understand the common points within the system in which energy losses occur. Surprisingly, roughly a quarter of the steam that is produced escapes the system before it ever reaches its intended loads. While recovering condensate, minimizing radiant heat loss and repairing steam traps are extremely crucial, they are just the beginning. Implementing techniques such as flue-stack heat recovery, deaerator-exhaust heat recovery and blowdown heat recovery also will help tighten up boiler plant operations.
New opportunities
Facility professionals should continue to push their teams to investigate new opportunities and never settle on a single set path. They must take initiative and explore their options and, perhaps, some of the suggestions covered in the new ASHE monograph will come in handy.
Kara Brooks, MS, LEED AP BD+C, is sustainability program manager at the American Society for Health Care Engineering; Peter K. Dahl, Ph.D., LEED AP BD+C & O+M, CEM, is principal of the energy and infrastructure group, HGA; Ryan W. Ollie, CEM, CMVP, EIT, is manager of energy solutions at Advocate Health Care; and Joshua Brackett, PE, is special projects manager at Baptist Health System.
Related Articles

Documentation of ITM for health care facilities
How to document inspection, testing and maintenance procedures and close the loop on compliance issues.

NFPA weekly update: July 27-31
Check out the latest updates on the National Fire Protection Association's Life Safety Code® and Health Care Facilities Code..

ASHRAE guidelines and standards open for comment
A list of ASHRAE addenda, revisions and drafts affecting health care open for public comment.