
Separating fact from fiction in ligature risk

In situations where 1:1 observation is not possible, ligature-resistance steps need to be taken instead.
Image courtesy of ASHE
Few events in health care facilities are as catastrophic — and preventable — as a patient suicide. Yet data indicate that suicide incidents are a serious problem, which suggests that hospitals must do a better job not only of identifying and monitoring patients at risk but removing the means to accomplish suicide in the physical environment.
The facts are sobering: The suicide rate has increased more than 25 percent nationwide from 1999 to 2016, per a recent Centers for Disease Control and Prevention (CDC) report, which also found that 54 percent of those who died by suicide in that period did not suffer from a mental health condition. According to the CDC, suicide is now the 10th leading cause of death in the United States, taking more than 40,000 lives a year. The most recent data published by the National Violent Death Reporting System (NVDRS) reveals that, in 2015, 83 suicides occurred in medical facilities.
The vast majority of these inpatient suicides have resulted from hanging, most commonly in a bathroom or bedroom and often using a door or its handle or hinge; a head, handle, bar or door in the shower; a ceiling or sink pipe; or another type of fixture as the ligature fixation point. Logic dictates that eliminating these and other ligature risks from the environment of a patient with suicidal ideation is necessary. Standards and requirements by accrediting organizations mandate as much.
But the truth is, many health care organizations are misinterpreting the requirements for reducing ligature risk. Others mistakenly believe that new ligature-resistance rules have been put into effect, which is not accurate. And plenty suffer from the misconception that eliminating ligature points is the only effective solution.
In reality, decreasing ligature risks isn’t practical in many hospitals. Additionally, it’s not the best or sole option. The key to more successfully preventing suicides is for health care organizations to change their way of thinking about this issue. They need to realize that ligature resistance is secondary to a more important priority: providing continuous one-to-one (1:1) observation of any patient with suicidal ideation.
The eyes have it
Continuous 1:1 observation of these at-risk patients should be considered the first priority of suicide prevention in hospitals. That’s because constant visual monitoring — especially observations conducive to 360-degree viewings by a paid sitter in the room assigned to one patient provides little room for error. Removal of objects that can inflict harm is also important, but there’s no substitute for human eyeballs and the ability to immediately intervene when suicidal thoughts change to a suicidal attempt.
Resources
The Centers for Medicare & Medicaid Services (CMS) attempted to clarify this point in December 2017 by publishing revised interpretive guidelines regarding the assessment of ligature risks. That publication stated: “Psychiatric patients requiring medical care in a nonpsychiatric setting (medical inpatient units, ED, ICU, etc.) must be protected when demonstrating suicidal ideation or harm to others. The protection would be that of utilizing safety measures such as 1:1 monitoring with continuous visual observation, removal of sharp objects from the room/area, or removal of equipment that can be used as a weapon.”
Put another way, if a person in the hospital can watch one assigned at-risk patient unceasingly, the only hazards that need to be removed are anything that could quickly be used to inflict harm. That means taking away items like glass flower vases, pens and sharp eating utensils. It doesn’t require major changes to the physical environment like eliminating grab bars, sink drain pipes or door hinges, or installing over-the-door sensors. There’s no pragmatic reason to take these steps, because an assigned sitter watching closely could easily intercede before a patient could achieve suicide.
In situations where this level of observation is not possible (as is often the case in psychiatric hospitals), ligature-resistance steps need to be taken instead. But if the facility is able to provide continuous 1:1 observation, removing ligature risks is not required, contrary to what many in the field are saying. The bottom line: Hospitals must do one or the other, but not necessarily both.
There are exceptions to this rule, however. Some states have privacy laws, for example, where patients are not allowed to be accompanied in the bathroom; in these instances, removing ligature risks is necessitated [see sidebar at right].
Another myth that needs to be addressed is that new ligature-resistance rules recently have been introduced. Technically, this isn’t true. What’s relatively new is that periodic visual observations of patients kept in a protective environment are no longer permitted by CMS. The health care field has learned the hard way that five-, 10-, or 15-minute checks on at-risk patients are woefully inadequate at preventing suicide. The CMS requirement of 1:1 monitoring with continuous visual observation replaces this practice.
It’s easy to see how that recent CMS edict has created confusion in the field. After all, it begs the question: If continuous 1:1 monitoring is in place, is ligature resistance still required? Rest assured that the answer is no — for now, anyway. CMS states that it’s working on drafting comprehensive ligature-risk interpretive guidance that should be released soon.
Action steps to take
To help their facilities reduce patient-suicide risks, it’s important for health care organizations to heed industry-accepted guidelines and best practices. Facility professionals are strongly encouraged to follow the American Society for Health Care Engineering’s (ASHE’s) three-step ligature-risk guidance for general acute care or emergency departments (EDs), by using helpful checklists and tools available and learning more about this topic.
In addition, The Joint Commission gathered a panel of experts in 2017 to offer direction on appropriate safeguards to curb suicide in health care settings. Following are summaries of many of the crucial recommendations the panel issued.
{kind=link}
Inpatient psychiatric units. First, to reduce risks in inpatient psychiatric units, it’s important to thoroughly assess the physical environment. Remember that safety provisions must be taken into consideration for any patient who could be at risk for suicide. To help matters, follow these recommendations:
- Make patient rooms, patient bathrooms, patient corridors and common patient care areas “ligature-resistant” (excluding nurses’ stations and the areas behind self-locking doors). Ligature-resistant means lacking points where a cord, rope, bed sheet or other material can be looped or tied to fashion a point of attachment that may lead to loss of life or self-harm.
- Use ligature-resistant hardware on doors between patient rooms and hallways. This includes, but isn’t limited to, hinges, handles and locking mechanisms.
- Make the transition zone between patient rooms and patient bathrooms ligature-free or ligature-resistant.
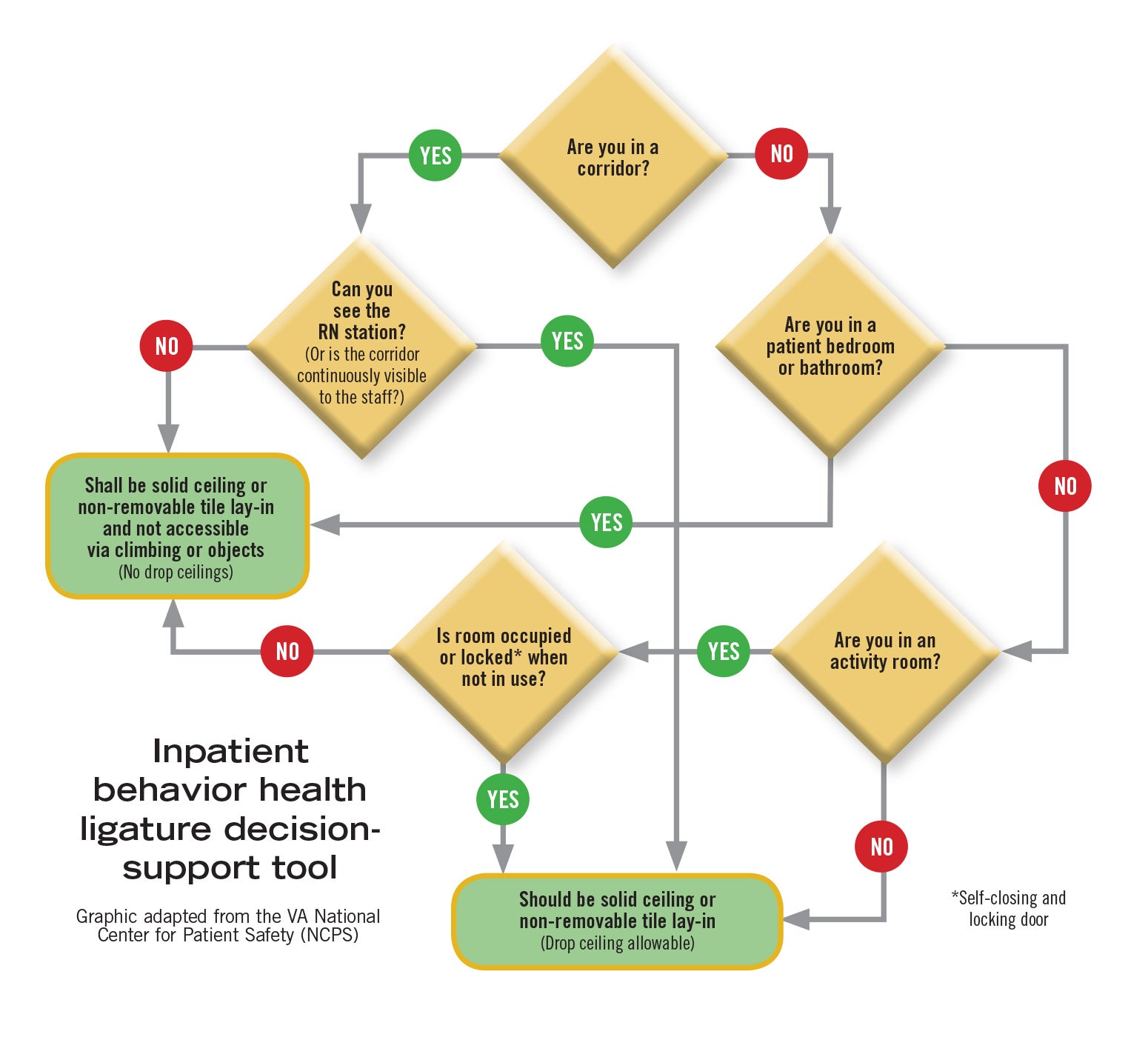
- Use solid ceilings in patient rooms and bathrooms.
- Use drop ceilings in common patient care areas and hallways, provided that all aspects of the hallway are fully visible to staff and there are no objects that patients could easily use to ascend to the drop ceiling, remove a panel and gain access to ligature-risk points above the drop ceiling.
- Determine the optimal type of patient bed utilized to meet both medical and psychiatric needs. Carefully assess and balance medical needs and the patients’ risk for suicide. For patients who require medical beds with ligature points, appropriate mitigation plans and safety precautions must be in place.
- Standard toilet seats with a hinged seat and lid shouldn’t be noted on a risk assessment or cited during surveys. They are not a significant risk for suicide attempts or self-harm.
- Organizations shouldn’t be required to install risk-mitigation devices to reduce the likelihood that the top of a corridor door will be used as a ligature-attachment point.
Emergency departments. When it comes to EDs, note that they don’t need to meet the same standards as inpatient psychiatric units to be regarded as ligature-
resistant settings. ED patients commonly need equipment and devices to treat and monitor their medical issues. Consequently, making the ED environment completely ligature-resistant is impossible. Still, organizations have to incorporate safety measures to protect patients at risk of suicide while they are being treated in the ED. Therefore, to reduce risks in this critical area:
- Place a patient with serious suicidal ideation in a safe room that is ligature-
resistant or that can be made so by excluding from the patient care area any fixed equipment that could function as a ligature point (e.g., a locking cabinet). - Remove all objects that present a self-harm risk that can be easily removed without negatively affecting the ability to deliver medical care. Implement policies, procedures, training, and monitoring systems to ensure that these are done reliably.
- Initiate continuous monitoring of a patient in a safe room (1:1 continuous monitoring, observations allowing for 360-degree viewing, continuously monitored video). Link the monitoring to the provision of immediate intervention by a qualified staff member when appropriate. Create a defined organizational policy that includes this detail.
- Fixed-ligature risks in the ED, including bathroom fixtures and doors, won’t be cited by surveyors.
{kind=link}
Medical-surgical spaces. As with the ED, the general medical-surgical inpatient environment doesn’t have to meet the same standards as an inpatient psychiatric unit to be considered ligature-resistant. It’s not possible to make this setting completely ligature-resistant, as suicidal ideation patients admitted to a med-surg inpatient setting typically require equipment to treat and observe them. Hence, to minimize risks in inpatient settings:
- Remove any objects presenting a self-harm risk that can be removed without negatively affecting the ability to deliver medical care if a patient requiring admission to a general acute inpatient setting has serious suicidal ideation.
- Employ and document any mitigation strategies, including 1:1 monitoring, careful evaluation of objects brought into the room by visitors and protocols for transporting patients to other parts of the facility, such as radiology. Implement policies, procedures, training and monitoring systems to ensure that they are done reliably.
- Fixed-ligature risks, such as bathroom doors and fixtures, won’t be cited in these areas by surveyors.
Staying informed
Hospitals can’t afford to take chances with patients who present a risk to themselves or others. The bad news is that each of these individuals needs to be closely watched with constant vigilance by a designated person. But the good news is that doing so forgoes the need to make costly, compromising and complicated modifications to the physical environment.
More Resources
- The Joint Commission expert panel recommendations
- The Joint Commission FAQ on "Ligature risks -assessing and mitigating risk for suicide and self-harm"
- The Joint Commission FAQs on suicide risk recommendations
- The Joint Commission Sentinel Event Alert on detecting and treating suicide ideation in all settings
- CMS "Clarification of psychiatric environmental risks"
- CMS "Clarification of ligature risk policy" (Dec. 8, 2017 memo)
- Behavioral Health Design Guide
Hospitals need to ensure that their policies, physical environment and staff are all on the same page. That means carefully reviewing and, if necessary, updating the organization’s policies and procedures, conducting thorough risk assessments and roundings, and training and drilling employees for suicide prevention.
It may seem easy to keep the setting safe, but it is more difficult than it appears. Items that can be used for self-harm are introduced into a hospital’s physical environment all the time, and it’s easy to overlook ligature points. Any one of these risks could result in a death or survey citation.
It pays to make a concerted effort to learn the facts and adopt best practices, especially until CMS issues further forthcoming clarifications. It’s also important to know whom to trust. Facility professionals can consider information from credible organizations like ASHE and The Joint Commission as gospel. On the other hand, they should take what they hear from consultants and colleagues based on past experiences with a grain of salt.
Finally, being better informed on this issue can especially help during a survey; it can position facility professionals to more effectively respond to a surveyor’s question, ask for clarification or even challenge a finding or citation when appropriate.
Chad Beebe, AIA, CHFM, CFPS, CBO, FASHE, is deputy executive director of the American Society for Health Care Engineering. He can be reached at cbeebe@aha.org.
Related Articles

Why portable weapons detection units should not be the default approach
Factors to consider when evaluating portable versus permanent weapons detection systems for healthcare facilities.

Building bonds is in our blood (and our brain)
Forming positive connections in the workplace will unearth the unique skills of each team member, allowing teams to work better together.
Preventing a possible outbreak through emergency response and remediation
Lessons learned from a real-life hospital flooding scenario and six steps for response.