
Navigating IBC and NFPA differences

Unifying the codes, standards and other regulations that apply to health care facilities is an ongoing effort of the American Society for Health Care Engineering.
Image by Getty Images
Over the past several years, health care facilities professionals all have heard the phrase “unified codes.” But what does that mean? A closer look at the two major codes organizations, some of their key requirements and their adoption trends illustrates the issues involved.
ICC and NFPA
The International Code Council (ICC) is the model code organization that develops and produces the International Building Code (IBC), International Fire Code (IFC), International Mechanical Code (IMC), International Plumbing Code (IPC) and others. These codes are updated every three years and are currently in the second year of the development of the 2024 editions.
In most parts of the country, the IBC and the associated fire, mechanical and plumbing codes are adopted at the state level or sometimes the local municipality level. These codes can be adopted frequently to stay up to date with the latest codes, or they may lag a cycle or two. Many municipalities also adopt modifications to the model code when they are adopted. These are usually referred to as local amendments.
Another model code organization familiar to all facilities professionals is the National Fire Protection Association (NFPA). The NFPA codes that facilities professionals are most familiar with are NFPA 101®, Life Safety Code®; NFPA 99, Health Care Facilities Code; and NFPA 70®, National Electrical Code®. Additionally, there are many other NFPA codes and standards used in the health care field.
The NFPA codes and standards are generally adopted by reference from the ICC codes. However, some states also adopt the NFPA codes as their fire code in lieu of the IFC. This generally includes NFPA 1, Fire Code, and NFPA 101. These two NFPA codes then reference several other NFPA codes and standards.
On a federal level, the Centers for Medicare & Medicaid Services (CMS) adopts NFPA 101 and NFPA 99. As with the building codes adopted by different states, the applicable edition can vary from state to state and from the edition adopted by CMS because the federal government typically updates the adopted version every 10 to 15 years. (It is currently using the 2012 edition, which it adopted in July 2016.)
Scope and differences
The scope of NFPA 101 is to address dangers to life from fire, minimum egress criteria and operations that are essential to life safety, including protective features and systems, building service and maintenance activities. Some requirements, although important to address fire conditions, also provide “ongoing benefit in other conditions, including non-fire emergencies.” The scope of NFPA 101 does not specifically include requirements for property protection, although many of the features that provide life safety also inherently provide property protection.
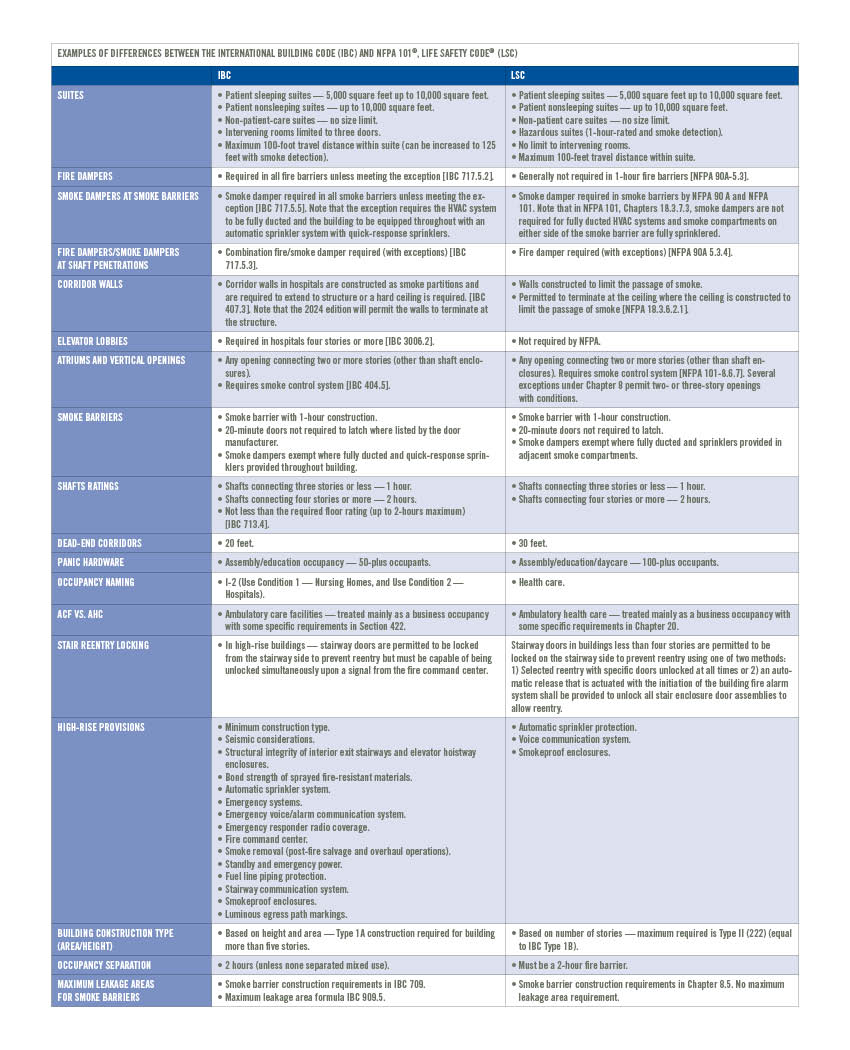
Examples of differences between the International Building Code (IBC) and NFPA 101®, Life Safety Code® (LSC)
Click image above to enlage
Unlike the IBC, which only applies to new construction, additions, alterations and renovations, NFPA 101 applies to both new and existing conditions. Even a building that was constructed many years ago and has not been renovated must comply with the existing chapters of NFPA 101, which establish a minimum level of safety for a given occupancy. In addition, unlike the IBC, which establishes the conditions on when a building is completed and ready for occupancy, NFPA 101 establishes operating conditions for a building after being occupied.
The IBC addresses many of the same requirements as NFPA 101, including minimum construction type, rated separations, interior finishes, means of egress, and fire alarm and fire suppression systems. However, the IBC also goes further to address natural disasters such as wind, flood and earthquake requirements, as well as accessibility requirements, minimum ventilation and safety glazing.
Another difference between the IBC and NFPA 101 is in the way they address occupancy classification and how they handle areas and spaces where high-
hazardous materials are present in significant quantities. The IBC has a separate occupancy classification for areas or spaces that manufacture, process, generate or store “materials that constitute a physical or health hazard” in amounts larger than what is permitted in control areas.
NFPA, on the other hand, does not create a separate occupancy classification; instead, there are provisions for high-hazard contents that must be followed regardless of the occupancy whenever applicable. High-hazard contents are “those that are likely to burn with extreme rapidity or from which explosions are likely.” Additionally, there are subclassifications of certain occupancies, such as storage and industrial, for those that store or use high-hazard contents. Within the occupancy chapter, additional requirements apply based on the high-hazard classification.
The IBC includes an additional occupancy classification: utility and miscellaneous occupancy. There is no equivalent in the NFPA occupancy classification. In the IBC, this is used for structures such as barns, sheds and towers. While there is no separate occupancy group for these in the NFPA classifications, these structures would still be assigned an occupancy classification.
Depending on how the space is used, storage, industrial or business occupancies are potential examples of appropriate occupancy classifications. Like the IBC, NFPA 101 has requirements for “special construction” and “high-rise” buildings that provide specific code regulations that modify the base occupancy requirements to accommodate these unusual surroundings or structures and the risks associated with them.
In the health care environment, NFPA 99 establishes criteria for levels of health care services or systems based on risk to the patients, staff or visitors in health care facilities to minimize the hazards of fire, explosion and electrical shock. NFPA 99 relies on the IBC, NFPA 101 or the fire code enforced by the local authority having jurisdiction (AHJ) for building construction and compartmentation, fire alarm and smoke-detection systems, and fire suppression systems. The IBC does not have a comparable document to NFPA 99. In the case of medical gases, the IPC references NFPA 99.
While not exhaustive, the table included in this article outlines some of the more significant differences between the IBC and NFPA 101. For a more extensive comparison between these codes, facilities professionals should refer to the American Society for Health Care Engineering (ASHE) monograph titled “Life Safety Code Comparison,” which compares the 2000, 2012, 2015 and 2018 editions of NFPA 101; and the 2015 and 2018 editions of the IBC.
Methods of development
The methods used by the two model code organizations (i.e., the ICC and NFPA) are both considered consensus code processes. However, the ways the two organizations develop the codes are very different. As previously noted, the ICC family of codes is revised on a three-year cycle and divided up to include different codes in three separate cycles (A-cycle: IBC, IFC, IMC and IPC; B-cycle: Administrative, International Existing Building Code and International Residential Code; and C-cycle: International Green Construction Code).
Anyone is permitted to propose a code change, and an ICC committee will rule on the proposal during the code action hearings. Based on the outcome of these rulings, anyone can submit a “public comment,” which is heard during the public comment hearings. At this point, only government employees (e.g., building and fire officials) are permitted to vote. The outcome of the public comment hearings is final and makes up the content of the next code edition.
Conversely, the hundreds of NFPA codes and standards are revised in a consensus process that includes a public input stage, where a technical committee reviews and votes on proposed code changes (which results in a first draft report); a public comment stage, where the same committee reviews and votes on public comments on the first draft report (which results in second draft report); and a final technical session, where any NFPA member can vote.
The outcome of the technical session will make up the content of the next code edition. However, any changes that occurred during the technical session are subject to an appeal to the NFPA standards council. Most of the NFPA codes and standards are on a three-year cycle, though some of the codes extend to a four- or five-year cycle.
Unification efforts
Now that the two major codes organizations and their development processes have been discussed, facilities professionals may want to know how unified codes affect them. Facilities professionals all are familiar with a local AHJ (e.g., building or fire official) requiring something to be constructed in accordance with one code and then a second AHJ (e.g., state or federal official) requiring it to be done differently. Generally, this is because of a difference between codes, such as a discrepancy between the IBC and NFPA 101. It also can be a difference between editions of the code where the two AHJs are enforcing two distinct editions (e.g., 2012 edition of NFPA 101 and the 2018 edition of NFPA 101).
ASHE’s ongoing effort to unify codes is intended to reduce the frequency of this scenario, and while significant strides have been made to unify the codes, there is still work to be done. The code adoption process that causes different editions to be adopted by different AHJs complicates this issue.
Those who would like to become more involved in helping to unify the codes and standards that apply to health care facilities should reach out to the ASHE advocacy team.
Post-certificate of occupancy differences between IBC and LSC
Key differences between the International Code Council’s International Building Code (IBC) and the National Fire Protection Association’s NFPA 101®, Life Safety Code® (LSC), have to do with the building post-certificate of occupancy.
While the IBC and LSC address construction of various use and occupancy types, the LSC and its referenced codes define inspection, testing and maintenance (ITM) requirements for installed systems and components. Adherence to these required codes and standards are fundamental to a building’s ongoing accreditation and compliance requirements.
Life safety drawings/plans is an area that typically shows differences between the IBC and LSC. It should be noted a life safety drawing/plan is required by an accrediting organization (AO). While AOs have differing requirements, minimum requirements should include:
- Areas of the building that are fully sprinklered (if the building is partially sprinklered).
- Locations of all hazardous storage areas.
- Locations of all fire-rated barriers.
- Locations of all smoke-rated barriers.
- Sleeping and nonsleeping suite boundaries, including the size of the identified suites.
- Locations of designated smoke compartments.
- Locations of chutes and shafts.
- Any approved equivalencies or waivers.
While these life safety drawing attributes have defined construction type (IBC) requirements by which they are to be built and maintained, it is important to denote in life safety drawings the use types (LSC). To clarify, a smoke barrier (use type) is to be built and maintained as a 1-hour fire-rated smoke barrier. If a life safety drawing defines this as a “fire” barrier, it and all its components (walls, ceilings, floors, ducts, dampers and doors) must meet this requirement. Specifications on life safety drawings can greatly impact design and operations, such as how a door must be rated and maintained. This one detail can, in turn, add considerable additional life cycle costs in the ITM process.
Where one sees this play out is in areas such as fire doors versus smoke doors and the correct use of dampers — whether fire damper or smoke damper types are accurate to the barrier or, in some cases, even required. In many cases, the use or occupancy has changed or migrated over time through various iterations of construction. Many of these rated devices are overrated for the current required use or occupancy type and therefore no longer required and could be decommissioned.
About this article
This is one of a series of monthly articles submitted by members of the American Society for Health Care Engineering’s member tools task force.
James Peterkin, PE, SASHE, is a senior fire protection engineer and code consultant at TLC Engineering Solutions, and Scott Mason, FRSPH, CHOP, CHC is a principal consultant specializing in enterprise strategic asset management with Brightly Software Inc. (formerly Dude Solutions). They can be reached at jim.peterkin@tlc-eng.com and scott.c.mason1@gmail.com.
Related Articles
ASHE helps remove requirements for unnecessary exit sign testing
After collecting member data and sharing it with the NFPA, ASHE's Regulatory Affairs Team successfully changed a requirement to save facilities managers hundreds of hours.
Local advocacy proves crucial to preventing undue burdens
While keeping an eye on national issues, ASHE's Regulatory Affairs Team also partners with members to advocate for state and regional matters.

Five compliance issues on ASHE's regulatory radar
ASHE's Regulatory Affairs Team highlights some of its advocacy priorities, what members should know and how to get involved.