
The EVS professional's role in managing old and new pathogens

The EVS team is on the front line of infection prevention and control.
Image by CloroxPro
Environmental services (EVS) teams have always been on the front line of infection prevention and control, but today’s threat landscape is shifting faster than many facilities can update their playbooks. Two high-priority emerging and reemerging pathogens — H5N1 avian influenza (i.e., “bird flu”) and measles — underscore a reality EVS leaders know well: the next disruption may come from a pre-vaccine era pathogen, a pathogen making the leap from animals to humans, or both at the same time.
Emerging and reemerging pathogen threats can be very disruptive. Not only can they bring fear of exposure, but the necessary enhanced cleaning protocols increase workloads and stress across the healthcare team and often bring fear of exposure. For these reasons, continuous readiness is key.
Measles is “something old,” a disease the United States declared eliminated more than 25 years ago but one that is quickly reestablishing itself as vaccination coverage has declined and outbreaks expand. In healthcare settings, measles is operationally disruptive because it is highly contagious, can linger in the air for several hours after a patient leaves and triggers resource-intensive exposure investigations that ripple across departments. H5N1 is “something new” in the sense that its current footprint is evolving. Ongoing spread in birds and other animals creates opportunities for spillovers to people, raising the stakes for early recognition and disciplined controls even though the current risk to the public is low.
While measles and H5N1 both trigger heightened infection prevention responses, they behave very differently in the healthcare environment. Understanding what is shared and what is distinct helps EVS leaders protect patients, visitors and staff while keeping essential services moving during investigation, isolation and cleaning.
The goal of this article is to translate these evolving threats into practical, EVS-relevant actions that strengthen readiness before a case arrives at a healthcare facility.
H5N1 and EVS
For EVS leaders, H5N1 can feel abstract until it isn’t. While seasonal influenza has a familiar operational rhythm, avian influenza introduces a different set of trigger points for readiness — the exposure history that raises concern for possible H5N1 infection, the additional layers of precautions that may be implemented and the need for cleaning to be both timely and meticulous. The good news is that EVS already has most of the core competencies needed. The key is knowing where H5N1 differs so EVS leaders can align staffing, personal protective equipment (PPE), products and workflow before a suspect patient arrives.
EVS leaders first need to know how H5N1 typically spreads. According to the Centers for Disease Control and Prevention (CDC), most human infections today are linked to animal-to-human transmission through contact with infected poultry, other birds or mammals. That means a suspect case often is identified not just by symptoms such as influenza-like illness, often with pink eye, but by a relevant exposure history such as farm work or contact with sick or dead animals.
Human-to-human transmission is possible but has been infrequent at the time of this writing. Only essential personnel should enter the isolation room. This puts a premium on early and clear internal notification. When the healthcare team flags a “suspect H5N1” evaluation, EVS leaders should expect enhanced precautions and confirm the plan for cleaning and disinfection with the infection prevention team before dispatching staff.
From an environmental standpoint, an important area of risk is high-touch surfaces. Like other influenza A viruses, H5N1 is an enveloped virus — among the easiest to kill through disinfection. However, the right product selection and contact time are essential.
Influenza viruses can survive on surfaces for hours to weeks, depending on the material, according to "Persistence of Pathogens on Inanimate Surfaces: A Narrative Review," published in the Feb. 9, 2021, issue of the online journal Microorganisms. The virus can spread when contaminated hands touch the eyes, nose or mouth. According to the CDC, special attention should be given to high-touch surfaces such as door handles, call light buttons and overbed tables. Coordination with nursing and ancillary departments also may be needed to ensure shared equipment, such as vitals machines, wheelchairs and gurneys, are cleaned between uses with an approved disinfectant.
Product selection is straightforward, but it needs to be verified. A healthcare disinfectant registered by the Environmental Protection Agency (EPA) that is appropriate for influenza A viruses from EPA List M should be used. Some products also may list a specific H5N1 claim. If the organism is not visible on the product label, EVS leaders should verify the master label (which can be found on EPA’s website) and ensure staff are trained to follow the stated contact time.
For EVS leaders, this is a moment to double down on process controls that prevent false completion, including standardized checklists for isolation rooms, appropriate contact time coaching, focus on high-touch points and targeted quality monitoring. For high-consequence pathogens, EVS should consider a supervised cleaning process.
The other H5N1 make-or-break area is the timing and thoroughness of terminal cleaning. Because H5N1 response includes airborne isolation plus contact precautions, EVS should confirm three things before entry: 1) whether the infection control team considers EVS as essential personnel for room entry for daily occupied room cleaning, or whether nursing performs this task; 2) the required wait time based on the room’s air changes per hour (ACH); and 3) the required PPE ensemble expected for EVS staff, which, according to the CDC, includes a respirator, eye protection, gown and gloves.
Once the patient vacates a room, unprotected individuals should not be allowed in the room until sufficient time has elapsed for enough air changes to remove potentially infectious particles. The room should undergo standard cleaning and surface disinfection procedures before reuse.
The bottom line is that H5N1 preparedness for EVS is less about reinventing cleaning and more about executing the basics flawlessly under uncertainty with clear triggers for escalation, appropriate PPE, disciplined high-touch disinfection and terminal cleaning that is paced to the room’s engineering controls rather than the unit’s urgency. When those pieces are in place, the EVS team helps turn a suspected or confirmed H5N1 event from a crisis into a controlled workflow that safeguards patients, visitors, staff and operations.
Measles and EVS
If H5N1 planning is about preparing for a low-frequency, high-consequence event, measles preparedness is about being ready for a fast-moving operational surge. Measles is one of the most contagious diseases seen in healthcare. It’s so contagious that up to 9 in 10 people who lack immunity and are exposed will become infected, according to the CDC. For EVS leaders, that level of transmissibility translates into a simple reality — small delays in identification or small gaps in engineering and cleaning workflows can quickly become large exposure investigations that disrupt throughput across the facility.
EVS leaders should anchor on two facts: measles spreads primarily through airborne transmission, and viable virus can remain in the air (and on surfaces) for up to two hours after an infectious person leaves a space, depending on ventilation. That persistence determines when EVS teams can safely enter, what areas require attention (not just the patient room) and how quickly a space can be returned to service.
When a suspected case is identified, EVS leaders should immediately connect with infection prevention and facilities/engineering teams to confirm the room’s ACH rate and the required time to clear airborne contaminants before EVS staff enter for cleaning without needing to wear a respirator. Depending on the ACH rate for the space, the wait period can be up to two hours after the patient leaves the room.
This also is where clear door signage and a documented “do not enter until” time can prevent well-meaning staff from inadvertently walking into a shared airspace too soon.
A recent resurgence signals why this matters now. In 2025, measles activity in the U.S. reached record levels, with 45 states affected and 96% of people who became ill reporting as unvaccinated. According to the CDC, as of May 15 this year, there have been 1,893 measles cases reported across 39 states and jurisdictions, which is well ahead of last year’s pace.
For hospitals, this pattern often shows up as higher volumes of “rule-out” evaluations in the emergency department (ED) and ambulatory entry points, where crowding, shared air and high-touch surfaces combine. EVS leaders should anticipate that measles response may extend beyond a single room to include waiting areas, triage bays, restrooms, elevator lobbies and transport routes.
On the environmental side, appropriate disinfectant selection is a must for measles. EVS leaders should use an EPA-registered healthcare disinfectant with an appropriate virus claim and not assume the absence of “measles” on a front label means the virus isn’t covered. Again, they should verify the EPA master label and ensure staff follow the stated contact time. Because measles response can involve multiple spaces cleaned under time pressure, EVS leaders should reinforce application technique, correct dilution (if applicable), sufficient wetness and a focus on high-touch surfaces in a deliberate sequence.
In surge conditions, EVS leaders should consider pre-identified airborne infection isolation rooms (AIIRs) and an EVS staging plan for supplies and PPE to reduce risk while maintaining throughput. They should consider only assigning measles-immune staff to cleaning these rooms. Finally, they should plan for volume — measles is disruptive not because cleaning is exotic but because the same steps must be repeated reliably.
Shared EVS protocols
Even though H5N1 and measles differ in how often they appear and how they spread in the community and in healthcare facilities, they intersect where the EVS team works every day — both can involve airborne risk in healthcare settings and both demand a coordinated response that pairs isolation practices with disciplined environmental hygiene. The most effective EVS programs build shared protocols that can be activated quickly, then fine-tuned to the specific pathogen once the infection prevention team confirms the scenario. These include:
- Screening and early signals. The EVS team doesn’t run triage, but it does help make screening workable. Respiratory etiquette stations stocked with masks, tissues, hand sanitizer and clear signage should be maintained at entrances, waiting rooms and other gathering points year-round. During periods of increased community transmission or public health alerts, EVS teams can support rapid placement of targeted signage, confirm availability of appropriate cleaning supplies and increase cleaning frequency for high-touch, public-facing surfaces such as door handles, registration counters, kiosks, chair armrests, elevator buttons and restrooms. The goal is to reduce environmental amplifiers while clinical staff focuses on identifying and isolating suspected cases quickly.
- Isolation, PPE and transport minimization. Because airborne isolation is central to both pathogens, EVS leaders should have a standing process to confirm 1) which rooms are negative pressure or AIIR-capable; 2) how negative airflow is verified; and 3) ACH rates to identify the airborne pathogen clearance time. When a patient must be moved, transport should be minimized and planned. Receiving areas should be notified in advance, routes with the least foot traffic should be used and prompt cleaning of elevators and touchpoints along the path should be planned. For EVS staff, the operational priorities are consistent — use the PPE ensemble specified by the infection prevention team for that room, limit the number of staff entering and avoid unnecessary reentry cycles by staging supplies and using checklists.
- Environmental cleaning and disinfection. In accordance with CDC guidance, EVS staff should follow standard precautions for routine linen and regulated medical waste handling with both pathogens. They should avoid shaking or agitating soiled linens, bag linens at the point of use and perform hand hygiene after glove removal. EVS staff also should “lean in” on high-touch surfaces. In real-world operations, transmission risk increases when time pressure drives partial wiping, contact times are shorter than the label requires and attention to shared equipment is inconsistent. A practical approach is to hardwire a high-touch sequence, then validate performance through coaching and routine auditing. For areas like the ED and waiting rooms, EVS teams should plan for higher frequency touchpoint disinfection during surges and after any suspect-case occupancy.
- Disinfectant claims, contact times and when sporicidals matter. EVS leaders should choose EPA-registered healthcare disinfectants based on the organism claim and the realities of the environment (e.g., surface compatibility, workflow and achievable contact time). For H5N1, they should use products on the EPA List M (effective for influenza A viruses) or products with an explicit H5N1 kill claim. For measles, there is no dedicated EPA list, so they should select a product with a measles virus claim and train to the correct contact time.
- Special considerations. Room reuse must respect the airborne component. Ideally, EVS teams should not be asked to turn a room until required air clearance has occurred, and completion should be documented so clinical teams can safely reoccupy spaces. For waste, routine streams from patient care areas are typically managed according to the standard process. However, an important exception may arise with H5N1 laboratory cultures, which should be handled as Category A infectious substance waste, which has a different regulatory pathway than routine waste. EVS and infection prevention leaders should confirm in advance whether the organization ever receives or generates cultures on-site and, if so, whether the waste vendor can support Category A handling and what training is required. Building these shared protocols before the next rule-out arrives helps EVS leaders protect staff while keeping patient flow and room turnover as steady as possible under pressure.
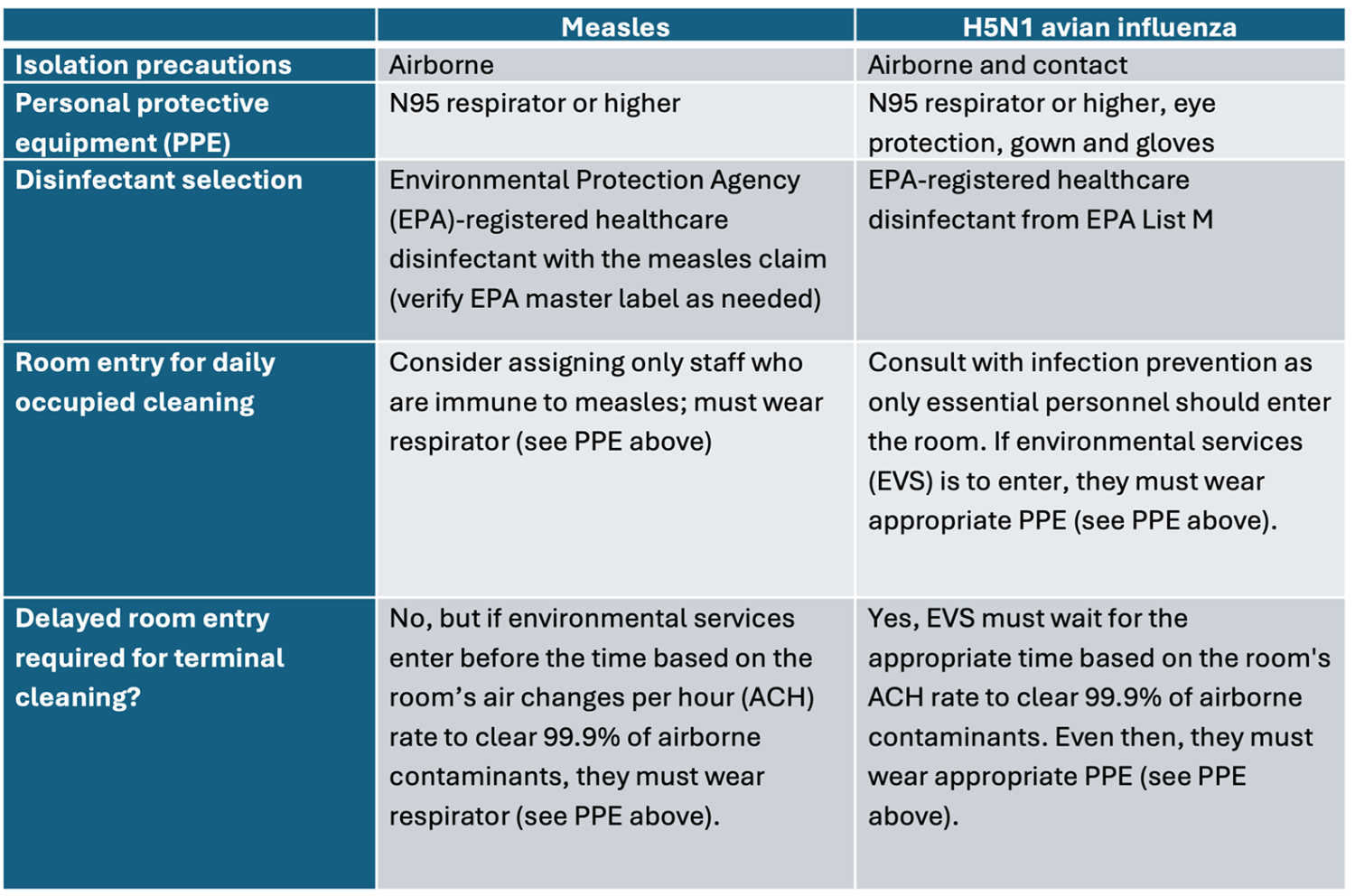
Click image to expand and view summary table of key infection prevention and control strategies.
On the front line
In an era of emerging and reemerging pathogens, the EVS team is not simply support to the infection prevention team — it is on the front line.
Both H5N1 and measles can contaminate high-touch surfaces and disrupt operations, but the difference EVS teams make is consistent — reducing risk through disciplined, repeatable environmental management. When EVS teams perform cleaning and disinfection correctly, adhere to required entry delays and room air-clearance timing, and document terminal cleaning with confidence, they help protect everyone in the healthcare facility while keeping beds and clinics available for care.
The key takeaway is balance. Some protocols are shared across both threats (e.g., screening support, airborne isolation readiness, PPE discipline, and rigorous cleaning and disinfection), while specialized details differ by pathogen (e.g., product claims, workflow triggers and special waste considerations such as Category A handling for H5N1 cultures).
Readiness requires planning, training, drills and the right resources — approved disinfectants with verified kill claims, clear contact-time coaching, respiratory protection and quick access to ventilation/ACH information that drives safe room reuse.
Looking ahead, emerging threats will continue to test healthcare systems, and EVS expertise will only become more valuable. EVS leaders should make ongoing education and protocol updates a routine maintenance task so the EVS team is ready to respond safely and reliably when the next "something old" or "something new" arrives.
About this article
This article is based on a presentation the author gave at the Association for the Health Care Environment’s 2025 AHE Exchange Summit.
Doe Kley, RN, MPH, T-CHEST, LTC-CIP, CIC, is an infection prevention expert at The Clorox Co. in Oakland, Calif.
Related Articles
ASHE helps remove requirements for unnecessary exit sign testing
After collecting member data and sharing it with the NFPA, ASHE's Regulatory Affairs Team successfully changed a requirement to save facilities managers hundreds of hours.
Local advocacy proves crucial to preventing undue burdens
While keeping an eye on national issues, ASHE's Regulatory Affairs Team also partners with members to advocate for state and regional matters.

Five compliance issues on ASHE's regulatory radar
ASHE's Regulatory Affairs Team highlights some of its advocacy priorities, what members should know and how to get involved.