
Utility service
 |
|---|
| Photo by David Stokes, courtesy of CBRE Healthcare Construction of a new central energy plant is well under way. |
Financial pressures are pushing health care organizations to invest in and leverage efficiencies in every facet of their operations.
Staffing efficiencies, technological innovations and procurement strategies all can impact financial performance, but no single strategy can lower operational costs more than a high-performance central energy plant (CEP).
Imagine a scenario in which energy savings of up to 60 percent can be achieved, sustainability benchmarks can be met, operational costs can be reduced and reliability can be improved.
It's possible, but getting there doesn't happen by accident.
Preliminary activities
Before starting the process of developing and implementing a CEP project, several preliminary activities should be completed. For instance, the organization must have completed a strategic master facilities plan in which a central plant retrofit or new central plant project has been vetted, approved and funded.
Many times a CEP is part of a larger capital project. However, to truly pass muster, the component initiative should be able to stand on its individual merits. Moreover, a solid business case must be made for the central plant to ensure success and executive buy-in.
Additionally, specific objectives and performance metrics should be established as guiding principles for the project. These can include targeting energy savings versus a baseline; targeting performance in U.S. Green Building Council Leadership in Energy & Environmental Design (LEED) ratings; adopting alternative and renewable energy strategies such as solar, geothermal and wind; incorporating energy innovation like combined heat and power; embracing design and construction practices such as integrated project management; and practicing active commodity management.
One further point of consideration is that the new plant must be designed with the future in mind. The health facility professional must consider other facility projects that are in the pipeline, how much future capacity should be included and how he or she can construct the plant while maintaining existing hospital operations.
Navigating the process
Once these preliminary activities have been adequately explored, researched and reported, the planning, design, construction and operations process can begin. This generally can be segmented into the following areas:
Planning. Much like a strategic master facilities plan is a 5- to 10-year road map for an organization, a strategic energy management plan can serve as a more detailed approach to developing a high-performance central plant. An energy management plan should contain the vision, business case, specific goals and responsibilities for the proposed project. It can be supported by additional tools such as a facility infrastructure assessment and an energy practice checklist, which can be accessed on the website of the Northwest Energy Efficiency Alliance's BetterBricks building initiative at
www.betterbricks.com.
One final piece of planning information is the health care facility's load profile. This provides critical data such as design and connected electrical loads, cooling capacity, heat loads, water consumption and other utility usage levels. The load analysis also is an important piece of information when conversations begin with utility providers and building plan reviewers because specific inputs may require utility distribution upgrades at the provider level.
Design. Armed with these tools, it's now time to start thinking about the design elements and how the information and ideas can be converted into a visual representation. Again, it is important for the facility professional to work collaboratively with the strategic master facilities plan to optimize placement, square footage and ultimate size of the campus. Understanding the LEED target and use of alternative and innovative energy initiatives will have a significant impact on the planned space, systems and infrastructure. Designing in a building information modeling (BIM) platform will help to minimize conflicts, streamline fabrication and maximize space utilization.
Designing a high-performance CEP is different from designing a functional central plant. Committing to a high-performance plant design means more than buying highly efficient equipment components. A high-performance CEP means developing a system that begins with design and proceeds all the way through operation and maintenance (O&M) plans to sustain the initial performance metrics over the useful life of the assets.
It also means working with an integrated design team of architects, engineers, construction managers, mechanical and electrical subcontractors, and commissioning agents. The purpose of the team and the integrated design process is to balance energy management with facility sustainability and internal climate control. One way to initiate the process is by scheduling an early design charette with the team. The meeting should be scheduled as a full-day workshop with follow-up meetings as required. Focusing on such areas as sustainability, performance metrics, energy programming, and core and shell modeling will yield productive material. Taken further, a deeper dive into lighting controls, daylighting, mechanical systems, ventilation and distribution systems will reap significantly larger opportunities for efficiency.
The goal of the charette is to make key decisions early to right-size the design and equipment for optimal performance while enhancing efficiency and supporting future growth. Sometimes this means paying a little more up front for equipment while balancing this cost against future energy savings. Too often, organizations will look at a simple payback methodology versus a full life-cycle cost analysis. Understanding when to use these different methodologies will help the integrated team to make better decisions utilizing the right information.
 |
|---|
A simple payback analysis is valuable when the first cost is relatively small, there is only one substantial life-cycle cost (i.e., electricity), the annual cash flow is fairly even, the equipment comparison is simple and off-the-shelf equipment is being installed. A life-cycle cost analysis is preferred when the first cost is relatively high, there are multiple life-cycle costs (i.e., gas, water and electricity), the annual cash flow has substantial variation, complex decisions impact other aspects of the project and the design will be customized.
The value of conducting the proper financial analysis and working in an integrated design mode can be visualized in the graph on this page.
Technology coordination. While most hospitals are familiar with building automation systems (BASs), building a new central plant affords the opportunity to leverage this system in a way that previously was not possible. Typically, a BAS has been used to monitor and troubleshoot all aspects of a central plant's equipment. Basic functionality includes maintaining set points and determining when variable-speed drives ramp up or shut off completely.
A high-performance central plant employs optimization software as part of the BAS logic. Using sophisticated algorithms, the optimization platform monitors real-time inputs from building loads and usage, as well as thermal comfort settings and automatically calculates equipment performance calibrations. In essence, this application functions as a type of artificial intelligence for all of the equipment and looks at the entire system rather than the sum of its individual components.
For example, current BAS technology can adjust the chiller motor and variable-frequency drives to function most efficiently given a predetermined control set point. Optimizing software goes several steps further in that it also directs the system to adjust the chilled water valves and variable air volume boxes in the HVAC system to economize air flow based on the thermostatic reading in a particular zone, so the efficiency of the total system is multiplied.
During the design phase, the team should determine the extent to which optimizing software will be used because this, too, can impact not only cost but also equipment selection. A commissioning agent also should be involved in this decision because he or she will assist in developing the sequence of operations for all equipment components and systems.
Construction. With the design work completed, the health facility professional can begin discussing the best way to deliver the end product. Assuming that he or she has incorporated the integrated team approach, the construction manager and selected trade subcontractors are already heavily engaged and are ready to build. Utilizing a BIM design platform now provides some flexibility in the construction phase.
One option is to "stick-build" the design on-site. The equipment has been specified, design coordination is complete and all that remains is to strategically schedule the work. Another option is to prefabricate the central plant and deliver it in a modular fashion [see sidebar, Page 26]. Regardless of the methodology, having completed the homework on the planning and design phases will make construction a cleaner affair with reduced change order costs to the health care organization.
If a facility professional is replacing an existing plant infrastructure, he or she should be sure to build a sequential timeline for disruptions related to the new project. It is important to schedule shutdowns with minimal impact to existing operations and still allow for maximum efficiency during construction. One method for controlling this process is to set a regularly occurring "disruption meeting" with the integrated team and key hospital operational personnel. The purpose of this meeting is to review the construction schedule of activities and any touch points with the existing infrastructure. It is important to include all stakeholders in these meetings to minimize complaints.
Commissioning. Commissioning should not be an afterthought to the process. Ideally, the commissioning agent (CxA) has been a part of the integrated team approach since the design phase. The CxA's initial role is to ensure that all of the equipment and system components work in harmony as designed, and to formalize the testing protocols prior to startup. Additionally, the CxA serves on behalf of the health care organization to ensure that intended operational usage is facilitated in the final product.
Commissioning also plays a key role in achieving a targeted LEED score. For example, to achieve a LEED Silver or higher rating, a CxA must be hired to perform enhanced commissioning services. This is not just a series of tests, checklist verifications and reports. Commissioning also sets the table for future operations. Commissioning scopes of work also should include a final O&M manual preparation as well as protocols for establishing the operational sequences for all of the equipment.
Measurement, verification and management. All of this work will get a health facility professional to a point where he or she has a functioning high-performance central plant. But, to achieve the long-term goal of sustainability and energy efficiency, especially the level needed to support the return on investment (ROI) goals laid out in the business case, the health care organization must invest in the ongoing maintenance of the system. This goes beyond the typical preventive equipment maintenance.
Historically, maintenance has been reactionary — something breaks and it gets repaired. To maintain the higher level of efficiencies within the system at the end of useful life, health facility professionals need to perform routine maintenance throughout the period of performance. Maintenance also must become predictive by allowing the facility professional to look at the available data and spot a problem before it occurs.
Trending analysis from the BAS will show when a particular piece of equipment is not functioning to its inherent efficiency capability. Rather than waiting for a catastrophic failure, repairs should be made as soon as the trouble is noted. This becomes obvious when measuring the cost of total future replacement against the maintenance cost in today's dollars. Moreover, the increased cost of operation calculated against the targeted energy efficiency even more convincingly justifies such intervention.
The role of the health facility professional is now more complicated. Beyond just keeping the system running, facility professionals also must have the proper tools in place to measure system performance. Additionally, they must be empowered to actively manage the efficiency of the central plant operations.
Above the norm
With advances in design capability, energy modeling, energy-efficient equipment and integrated delivery approaches, any facility is capable of achieving energy cost savings well above the norm. And while this may be implemented best with a new central plant, many of these considerations can be employed to leverage an existing system.
Even if an organization's most current strategic master facilities plan does not call for a new high-performance central plant, it is worth tasking the integrated team to consider such an option.
A new high-performance CEP may seem costly, but compared with the possible energy savings, the projected ROI should speak for itself. If the capital allocation process allows the organization to proceed, following these steps should enable health facility professionals to provide patients and staff with a high level of comfort and operate in an efficient manner.
David Stokes is a principal consultant at CBRE Healthcare, Richmond, Va. He can be reached at David.stokes@cbre.com.
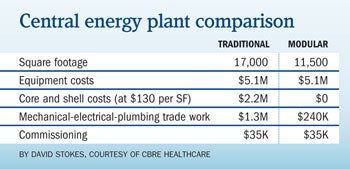
Modular central plants offer cost and space advantages
With the advent of building information modeling (BIM), 3-D design is allowing fabricators and integrators to assemble entire central energy plants (CEPs) off-site to be delivered in modules that can be bolted together and connected in the field.
There are several advantages to this approach, and the most compelling is cost. All of the pieces of equipment are built as modules and come complete within their own enclosure. The health care organization is immediately spared the cost of core-and-shell construction. Secondly, and also due to BIM and prefabricated assembly, the health facility professional can optimize the spatial impact and condense the same equipment into a smaller footprint versus traditional construction.
There are also less-tangible considerations. For instance, prefabrication in a controlled environment results in a cleaner and safer construction site, takes less field labor and encourages Lean production innovation.
Another considerable advantage is time, especially as it relates to construction scheduling. In many new construction projects, the CEP falls on the critical path. With the modular concept, fabrication of the CEP can begin at design completion, while early construction activities are getting started. In one recent project, the CEP was fabricated, delivered and connected prior to the hospital's being fully enclosed.
Additional advantages may be realized within the context of the specific regulatory environment. For example, the CEP in this project came with a master equipment label. As a result of this designation, the modular CEP did not count against the hospital's zoning coverage and certificate of need square footage calculations, thereby allowing the organization to potentially develop additional square footage on the campus.
However, there are also some downsides to the modular CEP approach.
First of all, most modular CEPs are not that attractive. They can be painted or hidden behind a screen wall, but at the end of the day, they truly fit the concept of form following function.
Second, to maximize the schedule advantage, the modular concept must be selected early in the design phase and there must be follow-through. Building programs must be developed early to capture the correct heating and cooling profiles. Decisions on equipment manufacturers must be made early, and the major mechanical subcontractor must be brought on early to assist in the procurement of the right integrator.
Related Articles

Students create cancer care center designs in just 48 hours
The 2026 PDC Student Design Challenge™ challenged students to create concepts of an oasis of care in the middle of a medical desert.

The facilities manager’s role in reducing healthcare-associated infections
From multidisciplinary communication to establishing safety procedures for construction, remediation and maintenance, facilities teams play a critical hand in reducing patient infections.

Intentional design, seamless care
Thoughtful wayfinding cues and a cohesive aesthetic enable smooth transitions between Endeavor Health Cardiovascular Institute's distinct occupancies.