
Six steps for planning low-voltage systems

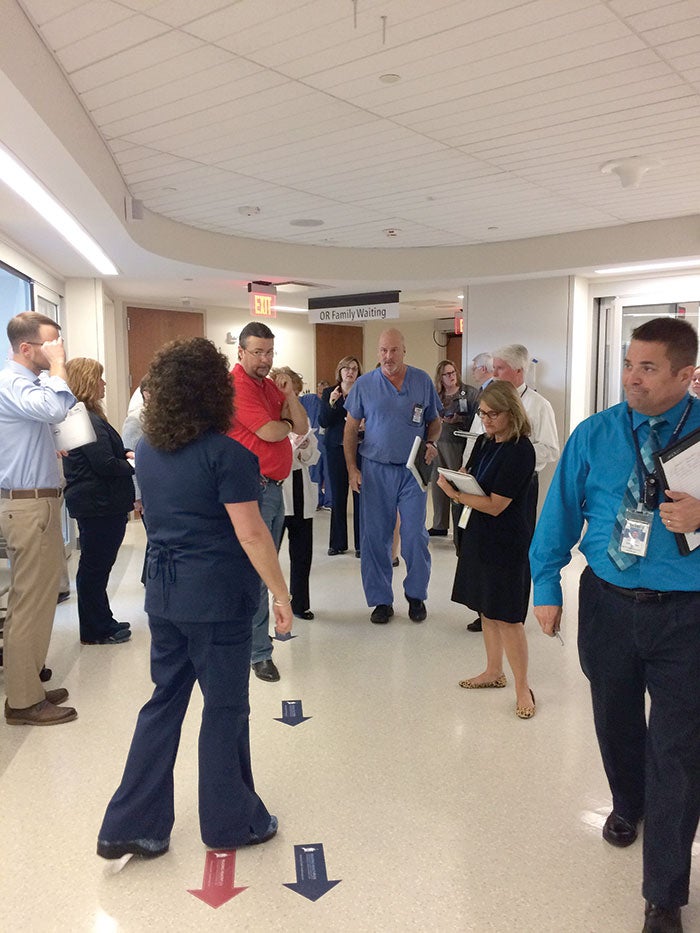
Due to compact space, staff accommodation needs and growing technology demands, operating rooms like this one in the Reading HealthPlex for Advanced Surgical & Patient Care at Reading Hospital in West Reading, Pa., benefit from well-coordinated technology integration.
With advanced technology being utilized in every corner of the hospital, early planning and end-user input continues to gain importance with regard to its integration during construction.
Due to its complexity and the interdependence of dozens of systems and components, technology integration requires a thoughtfully developed and carefully executed strategy.
Even with a growing trend toward standardization and open platforms, there are still many compatibility challenges to address in advance.
Low-voltage technology systems involve the transfer of data, audio and video, and include a wide range of applications: telemedicine, operating room integration, patient entertainment, nurse communication systems, patient monitoring, staff and asset tracking, security, master clock and dozens of others.
Technology planning that is too late and not well-organized can cost a project enormous time and money, as well as frustrate the entire team. To ensure a smooth technology integration, any new or renovated facility project will benefit greatly from these six steps.
1. Preplanning
The first step in the process is for facilities professionals to establish a technology steering committee, which is a cross-section of leaders who discuss the project while it is still in the concept phase. This committee should conduct vision-casting sessions, a method of summarizing the corporate vision for technology use and a growth strategy.
Many facilities already have an established technology steering committee but, for others, this may be the first time for all departmental leaders to be in the same room together to talk about technology. The value of this exercise alone cannot be overstated. This committee serves as a vision and leadership team to align the corporate vision, budget and strategy.

Members of this committee should include representatives from information technology (IT), clinical informatics, operations, nursing, medical, biomedical and facilities. Additional members can be engaged as the need arises. Facilities professionals then should begin outlining the technology budget. This budget can be anywhere between 10 and 15 percent of the overall project budget. Projecting parameters and guardrails early in the budget process will help to facilitate discussions in the user meetings and align the vision and the reality of the technology plan.
2. Planning
The next step is to hire or appoint a technology planner. For optimal results, facilities professionals should dedicate someone with the skill and experience to conduct the planning and execution of the project’s technology integration. It is critical that the project have dedicated leaders with significant knowledge and time to focus on managing the technology planning, procurement, construction administration and commissioning.
The technology planner can come from the hospital’s own staff, as long as that person has the requisite experience and can be released from his or her previous responsibilities to focus solely on this job for the duration of the project.
A benefit of using an outside technology planner is his or her awareness of options, new trends and industry pricing. People working in health care environments often are too busy to research new technologies and, given the rate of technological change, hospitals need someone who can eliminate the noise and provide clarity about appropriate technology choices and the pros and cons of each.
You may also like |
| Converging infrastructure technology systems |
| Medical grade wireless infrastructures |
| Hospital technology system commissioning |
|
|
Many hospitals realize the importance of a technology planner only after much of the potential benefit has been lost. Hiring or appointing a technology planner early saves an enormous amount of stress and frustration, and will pay for itself by avoiding change orders.
“Five years ago, we occasionally had a technology planner involved with our projects,” says Jay Hornung, ACHE, president of Healthcare Building Solutions, Langhorne, Pa. “Today, we see a technology planner on every single project.”
After a technology planner has been appointed, health facilities professionals should then hold user group meetings that involve all departments affected by the new construction, to understand their technology requirements.
In face-to-face meetings, the technology planner asks each group, “What do you need the technology to do for you to do your jobs well?” All input is documented so that design incorporates the technology needs of the users. User groups should include nursing, pharmacy, physicians, environmental services, respiratory therapy, admissions, nutrition services, chaplain services and all ancillary services.
User input is critical to success. The health care field reaps huge benefits from incorporating the voices of nurses and other end users in the design process, including fewer change orders, improved clinical morale, and better workflow and patient experiences.
Technology design incorporates the wants and needs outlined in the schematic design narrative and budget requirements.
Robert Goss, AIA, senior associate architect with Ballinger, Philadelphia, says his firm continues to find great value in consulting end users about new spaces. In addition to traditional field trips to other facilities to see new technology at work, Ballinger uses mock-up rooms and 3-D modeling, and recently has started using virtual reality to help end users experience proposed designs and solicit their feedback. “Virtual reality is the next big thing, because we can create a virtual room faster than we can build a mock-up room, and feedback can be incorporated more quickly as well,” he says.
Based on information gathered from the vision-casting sessions and user-group meetings, levels of need will emerge as “must have,” “should have” and “would like to have.” This process includes examining existing infrastructure to determine if it can be kept and expanded for use in the new construction. This is a good time for the hospital to identify preferred vendors — those the hospital already knows well and would like to work with.
The budget can be refined based on the levels of need. What initially started as a “would like to have” item might get placed in a future capital project to make room for more “must have” items. With a solid budget in hand, the health care organization can decide which level to build.
Determining who will be responsible for every part of the technology planning process will prove infinitely helpful as the process unfolds. Knowing in advance who is in charge of what through a responsibility matrix reduces needless finger-pointing and action-item neglect. Color coding the matrix makes it easy to see where the project may be falling behind.
3. Design
A schematic design narrative summarizes the hospital’s expressed technology wants and needs. It is drafted by the technology planner and handed off to the health care organization, architect and engineers for integration into architectural and engineering plans. This narrative also should receive sign-off from the technology steering committee.
In conjunction with the architect, engineers and the health care organization, the technology design incorporates intentions outlined in the schematic design narrative. In this stage, the technology planner ensures that end-user input continues to be reflected in the final design and adherence to the budget is maintained. Infrastructure often is designed to a higher need than will initially be utilized, so that future expansion is faster and less expensive.
The previously created responsibility matrix should be used to keep the project on course.
4. Procurement
With an approved design, the technology planner can write and distribute requests for proposals. Again, any preferred vendors should be included in this process. The outside technology planner’s knowledge of the marketplace will provide value here, because he or she will have worked with a broad field of vendors.
Consulting end users during the technology planning phase will save the owner significant time and money. The end users should come from all departments that will touch the technology.
All selected vendors must be able to work with each other. This critical concept should be established as early as the preplanning stage, so that everyone understands the importance of collaborative technology. All considered vendors should be collaborative and work as a team with the shared goal of a successful facility. This extends to the nature of their hardware and software, which should offer flexibility as needs change and ensure interoperability with other vendors’ products. Selected vendors must be willing to accept that there will be modifications in system parameters and requirements during and after construction as all the players merge into one system.
Reviewing bids and vendor interviews should include simulations with vendors on the short list to demonstrate features and performance with multiple user groups. Contract negotiation, warranties, end-user education and training, and support must be considered for each new technology and vendor.
5. Construction administration
Facilities professionals must effectively manage requests for information. Communication among members of a construction team can be complicated and confusing. A good technology planner will keep all the threads straight and will bring useful tools for streamlining and answering information requests.
When a change request is initiated, there needs to be a solid approval process, because there are a number of documents that will need immediate updating to keep the project on course. Even a momentary lapse in this process can result in expensive mistakes. Justification and documentation must be in place through the approved process to proceed.
Additionally, facilities professionals should conduct regular site visits during construction to ensure that the contractors and vendors are following the design plans. The regularity of these visits will depend on the complexity of the project, and may range from once a month to a permanent on-site project manager for the duration of construction, testing and training.
Finally, concluding patient care in the old facility and launching it in the new facility is not an instantaneous event. The ramping down of one and the ramping up of the other must occur simultaneously and with great attention to a number of details. Hiring a transition planner with experience in what is almost always the turning off of an older, outdated facility and turning on a far more technologically advanced one is critical to a smooth transition.
Adequate preparation and training for work in the new facility is essential and a transition planner has the specific experience — including speaking the “language” of all health care departments — to educate all employees on navigating this process. Budgeting for this kind of planner will result in the smoothest and safest transition possible, and one that gives clinical, IT and biomedical staff time to become masters of the new space, equipment and systems.
“For a year or more on larger projects, this position will be a full-time job,” Hornung says. “The amount of communication, data tracking and attention to detail demands that a hospital not try to add these responsibilities to an existing employee’s workload.”
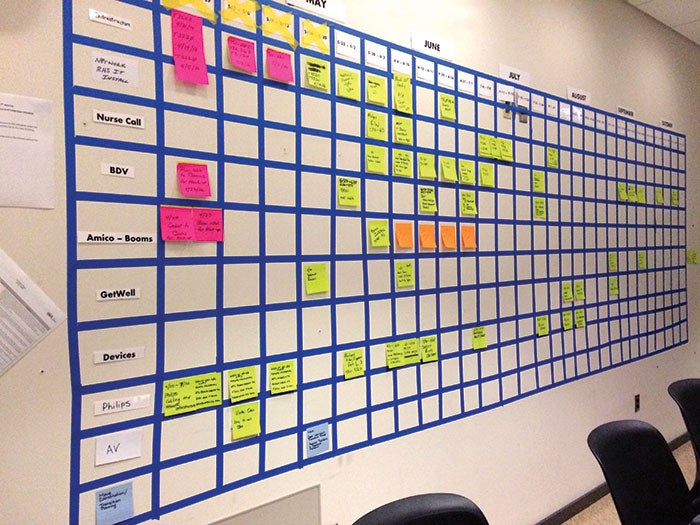
A responsibility matrix, shown here as an enlarged wall chart, is used in weekly meetings that keep team members informed and holds them accountable.
Weekly meetings led by the technology planner keeps everyone informed and accountable. The responsibility matrix is useful during these meetings to keep the project firmly on the rails and inform all team members of the status of all parts of the project. An additional benefit is the accountability it provides, as items that are past due can be communicated with a highly visible color to call attention to the lapse.
6. Post-installation
Facility testing must begin well before occupancy using the staff who eventually will run it. There may even be weeks or months of overlap to allow all team members sufficient hours in the new space to ensure a smooth opening.
The ramping up of the new facility doesn’t end when the doors open and the first patient is treated. It continues for several months while all the wrinkles are smoothed out and employees have their first real experiences in the new space. This is especially true for clinical, IT and biomedical staff who will not encounter every common adverse situation in the new space for perhaps a year after opening.
Regular access to commissioning resources for six to 12 months is important so that hospital employees have a consistent person or small group of people who can answer questions and work through problems.
Facilities professionals should keep user groups intact so that they can continue to give feedback on the space and how it’s working. Because they have been involved all along, they will be more invested in the facility and better equipped to provide useful feedback. They may be able to help avoid expensive change orders because they are more knowledgeable about the entire system and can spot simple solutions better than they could have when they were not involved.
Conducting a post-occupancy review six months to a year after activation will ensure that proper workflow, efficiencies, technology optimization and quality measures are in place and sustainable.
Careful implementation
Low-voltage, advanced technology systems are crucial for the safe and efficient operation of modern health care facilities.
A carefully considered implementation program encompassing the key steps of the project will ensure that such systems will meet the needs of staff and patients.
Debbie Gregory, DNP, R.N., is senior clinical consultant with Smith Seckman Reid Inc., Nashville, Tenn. She can be contacted at dgregory@ssr-inc.com.
Related Articles

Health system invests millions in high-tech beds
NYC Health + Hospitals' upgrade marks a systemwide enhancement to patient comfort and care.

Agencies issue eight principles for OT cybersecurity
U.S. and international agencies released eight principles to eliminate cyber vulnerabilities in operational technology.

NFPA report reviews risks associated with smart buildings
The NFPA's Fire Protection Research Foundation report dissects the impact of smart building technology on life safety and presents a roadmap to address its challenges.