
Planning outpatient health care facilities

Resilient principles of modular planning and flexible infrastructure were employed in Wexner Medical Center Outpatient Care New Albany in Westerville, Ohio.
Photo by Kevin G. Reeves
What if architects thought differently about how they design and build structures used for outpatient services? If the health care field has learned anything from the past two years, it is that immediate change will happen whether the field is ready for it or not. Often when change happens, there is a reaction or overreaction that promulgates a solution that may not be necessary.
Change will continue to occur and can be driven by a series of factors, not necessarily one cataclysmic event. Thus, architects must design for the unexpected, allowing for adaptability when the inevitable happens. These goals of resiliency and flexibility must address both the ability to maintain operations and limit downtime amid a change event, providing a reasonable value proposition to health care organizations.
Change agents and trends
Change agents that originate from within the field and from uncontrollable external forces have resulted in operational impacts affecting health care. Health care changes over the past 25 years include expansion of decentralized outpatient services away from acute care campuses. This change is driven by consumer expectations, consolidation of health care providers into systems and the competition for market share in growing population centers.
The landscape is seeing new facilities, ranging from outpatient clinics and ambulatory surgery centers to health care in retail outlets such as Walgreens, CVS, Walmart and Costco. The advent of the iPhone era that began 15 years ago and the explosion of technology have impacted every aspect of both home and business life. The impact to the health care field has led to minimizing or eliminating paper records, improved and created new diagnostic tools, bolstered the connectivity that has supported more complicated and emergent treatments in the outpatient venue, and brought virtual care directly into the homes of patients.
Likewise, over a period of 25 years, external forces such as natural events, economic trends and emerging medical conditions have also left their mark. The increased likelihood and frequency of natural or manmade disasters prompt surges in health care needs, and disaster responses are regular and ongoing occurrences that show little abatement.
Technological tools and apps have become part of the mental and social well-being of young and old alike, leading to an awareness and recognition of mental health needs. Sociomedical issues of opioid abuse, public health concerns and continuing growth of chronic diseases have not been abated by the ubiquitous knowledge of their impact.
Lastly, the U.S. has learned that a virus can stop the world in its tracks as witnessed during the past two years. There are resultant supply chain disruptions, global market volatility, inflation, energy costs and an economic recession — the fourth in the past 30 years.
While such events have occurred throughout history, the acuity and magnitude have grown proportionally and have a greater impact across a connected world. These factors have operational impacts on all fields, including health care and the design and construction industry. Thus, health care architects stand at a generational moment that requires a different way of addressing the opportunity before them.
Resilient design and construction
As with any change, the design process and components that embody design must each be considered with the same rigor. This starts on a macro scale and works sequentially to the details to ensure function and operations align with programmatic requirements. It issues a challenge to consider alternate approaches to the commonly accepted standards in the interest of producing better outcomes.
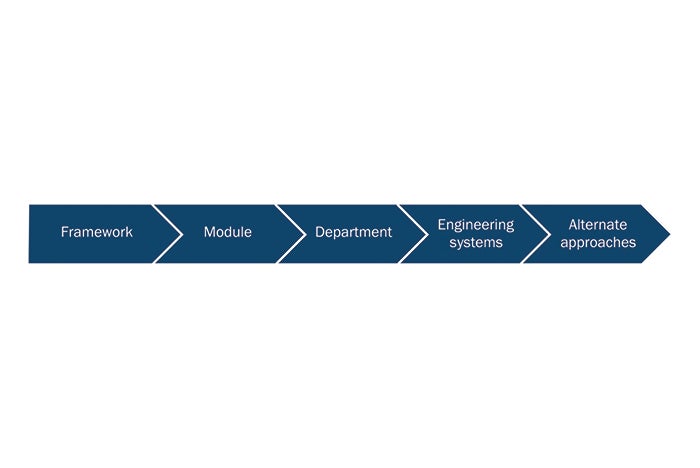
Framework. A resilient design model is flexible and adaptable to unanticipated needs. Such a model avoids the kind of specialization that freezes infrastructure and space requirements to a moment in time, a particular technology or a personal preference. Agnostic space planning holds to the idea that specialization of departments can be driven by institutional preference rather than need. Thoughtful consideration must be given to proximity and size of utility chases, exhaust ducts and other infrastructure pathways originating in the building core. Core elements are fixed vertically and organized in a horizontal distribution to allow maximum adaptability and expansion.
Designing flexibility and future capacity into the system, regardless of present departmental ownership, leads to success in resilient planning. Specific rooms can be planned with capacity for future utility and technological expansion. These spaces are adaptable to different layouts, care delivery methods and modalities. Flexible spaces such as these are designed with an inherent agnostic attitude towards the specialty inhabiting them at any given time. Such rooms are more infrastructure-intensive than typical exam or office spaces and must be sized adequately and placed appropriately in a building.
Equalitarian modularity. Equalitarian modularity suggests uniformity is a key word to simplifying design and reducing the customization of elements. Uniformity is not the enemy of design but the clarifier.
- The first requirement of a resilient planning concept is the module. The module can be defined by the predominate room type, such as a 10-foot-by-12-foot exam room in an outpatient setting. If room types require a larger or smaller footprint (based on regulatory guidelines, equipment or user preference) they should be sized up or down to align with the module. Regardless, each room type in the program should be a multiple or division of the module.
- The second requirement of resilient planning promotes the benefit of a space-driven program as opposed to a program-driven space. Support spaces, shared functions and administrative spaces should be equally distributed in proportion to the number of treatment spaces and not repeated for every department.
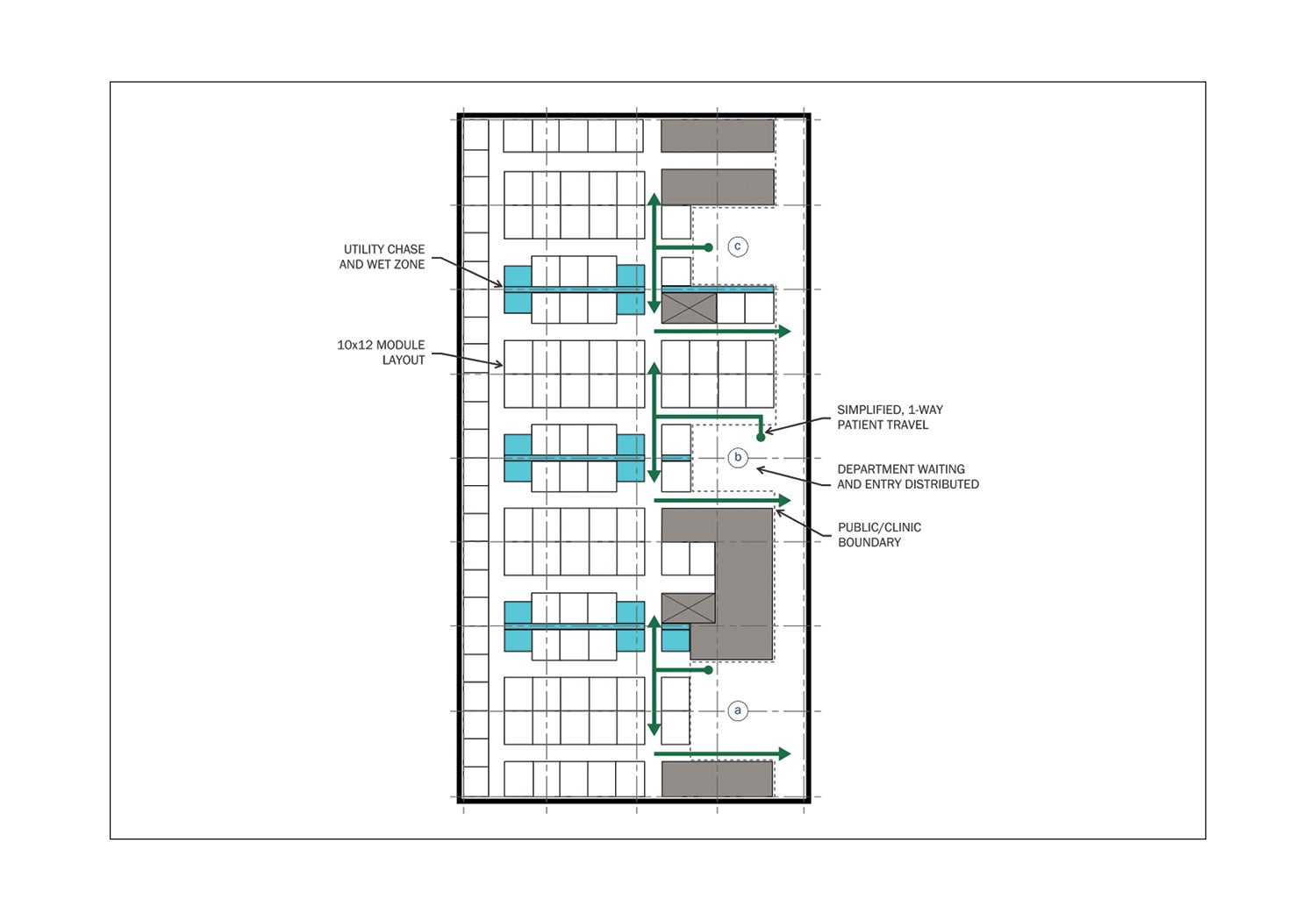
- The third requirement is a simple, rhythmic circulation system that promotes intuitive wayfinding.
- The fourth consideration is applying a similar rigor to the integration of engineering systems and infrastructure design. With room templates, wall and ceiling devices are placed in consistent locations for repeated rooms, which allows for a uniform layout of distribution and similar lengths of distributed elements. These elements include HVAC ductwork, electrical conduit and wiring, and plumbing piping. Quantity of devices per planning module also are consistent, and the head-end systems are scalable to known quantities.
Head-end systems, such as HVAC air-handling units, should be selected for scalability and be variable in capacity. This allows for variation in program in any one module. Variable air systems are common in health care, but they often are customized to the initial program use. If variable systems are sized for a more demanding use, they are capable of modulating to lesser demands and are more efficient when partially loaded. The required increase in capacity for head-end systems and distribution to handle more demanding programs within a percentage of planning modules must be balanced with efficiency gains in distribution layout, reduced distribution losses and increased flexibility for future modification.
These concepts allow for flexibility when the latest disruptor in health care arrives. Content is more critical than area and simplifying a plan according to a module allows for more creativity within the room boundary. This simple approach avoids customization at the cost of flexibility, which will be necessary as soon as the newest equipment model is released or there is management turnover.
Room standards support the simplification of design, ensuring that finishes and utilities are deployed equally in all occurrences of a single room type. A typified room allows clarity of design intent, repeating finishes and branding elements consistently, removing the temptation for intense and unnecessary customization in every room.
Designers can focus on a few options that align with brand standards and design aesthetics. Less attic stock and maintenance specialization are required by simplifying finishes; furniture, fixtures and equipment; and lighting selection. Changeable elements such as furniture tolerate fluctuating trends and tastes and offer opportunities for a quick refresh.
Crossing all disciplines
Design considerations cross all disciplines and speak to the emotional needs of occupants. The neighborhood is a relatable organizational concept that allocates space for essential services and occupant comfort.
Architecture. Uniqueness within uniformity is achievable through a creative design process and a site-specific response. Just as neighborhoods have zones for housing, shopping, services and outdoor space, so must a clinical facility have similar considerations.
Each clinic, from imaging to family medicine, has a certain base program required for it to function. This base program includes administrative space, patient care areas, utilities and storage. These common elements are defined in the programming phase and distributed through the modular plan.
Distribution of these elements is important for the future of the clinic, as department boundaries may flex and what is currently assigned to serve one department may well serve another in the future. Designing support spaces that are agnostic to a specialty will help a facility adapt to new demands from market fluctuations and demographic shifts.
Planning for a fully functioning neighborhood of clinics ensures that, no matter who moves in, basic infrastructure and space needs are met. This takes the pressure off the institution, which may be considering modalities at a particular facility or juggling leased space elsewhere.
An agnostic, modular plan that treats clinics in a “small, medium, large” fashion with respective support programs can easily fill in the blanks of the who and what later. This flexibility is critical to successful preparation for inevitable change and is the foundation of a resilient planning model.
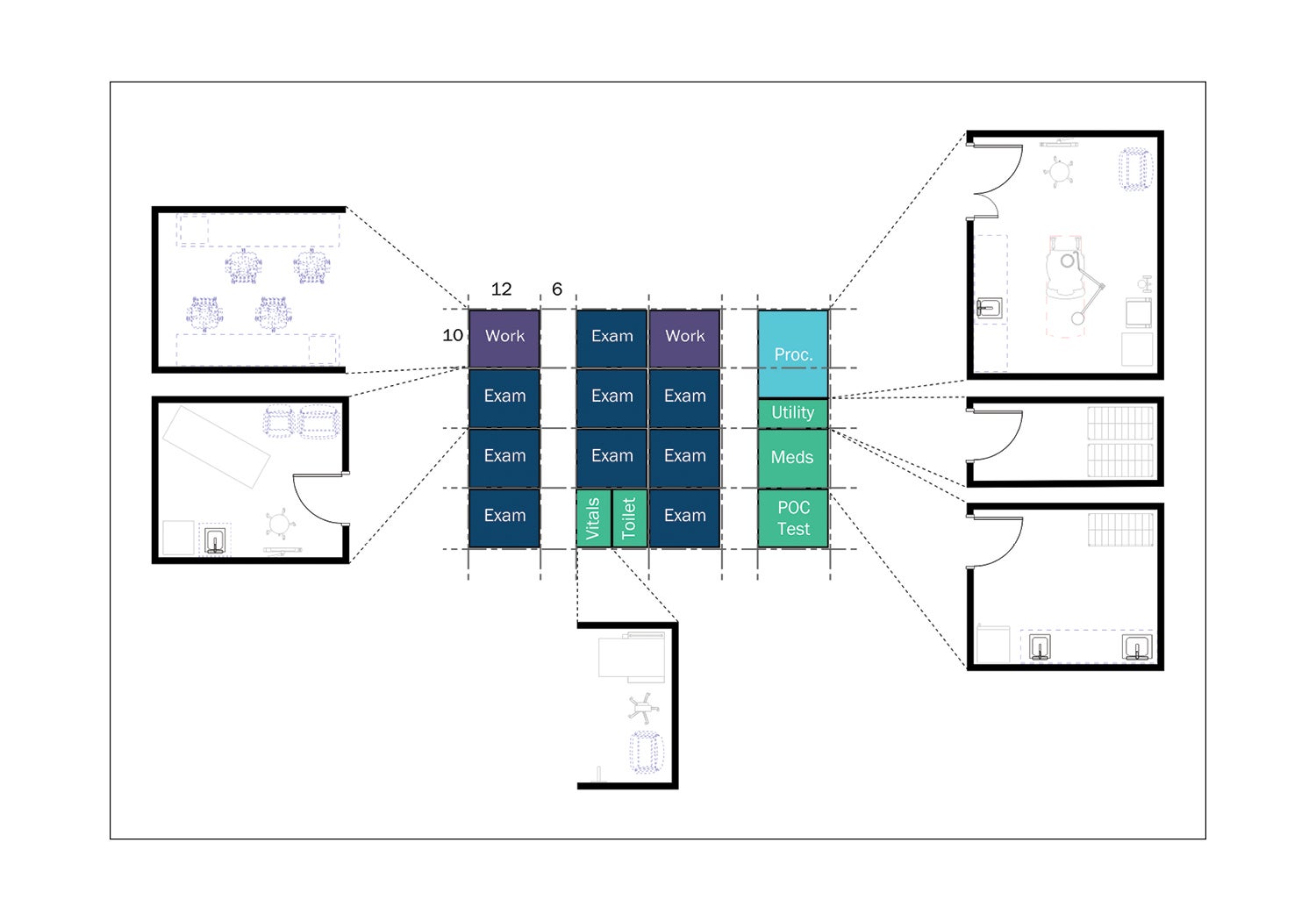
Click image to enlarge and for caption
Engineering systems. Considering engineering systems are approaching 50% of the cost of a medical facility, the same rigor and coordination with the architectural design must be addressed simultaneously. To allow for flexibility in planning, building structure must maximize a clean floor plate. Vertical core elements logically located and spaced on grids consistent with planning module dimensions allow for limited interruption. Deeper horizontal structural elements located between planning neighborhoods clear the path for horizontal distribution of other systems within the neighborhood.
Horizontal distribution organized into utility highways or spines above corridor ceilings allows flexibility in space configuration on either side of the corridor. Grid distribution from vertical shafts at centrally located cores minimizes the size of horizontal elements such as ductwork, and centrally located electrical and technology closets reduce the radius of distribution. This allows for flexibility in program and improved system performance. For stacked planning modules, the decision of same-handed rooms versus mirrored rooms should be evaluated in totality, taking into consideration the operational benefits, ability to prefabricate and construction strategies to address distribution risers within the modules. Additional height within the first level ceiling space can accommodate horizontal plumbing distribution mains and, for taller buildings, additional height may be built in at intermediate levels.
Neighborhoods can have similar heating and cooling loads because of similar space use, but certain program elements or features can disrupt uniformity in HVAC distribution. For example, when neighborhoods have modules located on exterior walls, exterior zones can have higher load and airflow requirements. A high-performing envelope will help reduce this variation. Elements such as labs or imaging rooms also require special consideration. These spaces tend to have higher loads due to equipment and, when located within a neighborhood with otherwise standard treatment, will challenge the uniformity of the air distribution systems. To respond to these needs, distribution mains should be sized to accommodate a percentage of these elements to preserve the standard grid and allow for future flexibility in space use.
For more acute care or specialized departments, separate air-handling systems for the department neighborhood can improve operational efficiency as the system can be controlled to the specific needs of the department. These systems are usually tailored to the specifications of the initial program for filtration and air change requirements, rather than being designed to be department agnostic. Another approach is to provide systems capable of a range of operation and that fit with a range of features, such as higher efficiency filters, so the units can serve a range of programs. This would result in a uniform layout of similar units that are variable in capacity and adaptable in features.
Alternate approaches
While design considers the perpetuity of the built environment, the need to provide for change, flexibility and expansion must be considered in every design effort. In a similar way, the approach and process of construction must be integrated into the design process from the outset.
Click image to enlarge and for caption
The idea of modularity and equalitarian planning can be extended to the construction process. The concept of prefabrication is not a new idea, but its use is growing in response to the demand and desire to reduce waste, improve quality, leverage the available work force and shorten construction schedules.
The availability of skilled labor, variation and availability of building materials, accelerating construction schedules to avoid escalation and bringing product to market sooner are all strong considerations to use prefabrication and Lean building principles throughout the design and construction process.
The rigor of modularity increases the number of elements that can be prefabricated. This becomes acutely relevant in the installation of engineering systems. Prefabrication reduces on-site labor, improves quality because systems are installed in a controlled environment, and allows for tighter tolerances to produce a more compact layout.
Utility highways can be prefabricated into racks and consist of elements from several trades. These racks are most effective with the uniform distribution that can result from planning modules.
Engaging change agents
Change happens on all fronts: health care delivery, patient needs, impacts from external factors, planning and design processes, construction delivery methods and technology.
The built environment incurs a significant investment in time, resources and finances, giving greater weight to the concept of designing for resiliency and flexibility. This is not suggesting a single solution or prescriptive design manual. However, it does suggest a greater collaboration between health care providers, vendors, designers and the construction communities to develop these ideas.
Beyond that, because design is agnostic, this also is a call to reach outside the architects’ first ring of influence to engage political, societal and regulatory agents; higher education partners; thought leaders; and parallel fields that create obstacles on the path to achieving meaningful change.
About this article
This feature is one of a series of articles published by Health Facilities Management in partnership with the American College of Healthcare Architects.
Philip LiBassi, FAIA, FACHA, is senior principal; Elizabeth Dolinar, AIA, EDAC is associate; and Jason Majerus, PE, is principal and senior engineering leader at DLR Group. They can be reached at plibassi@dlrgroup.com, edolinar@dlrgroup.com and jmajerus@dlrgroup.com.
Related Articles

The facilities manager’s role in reducing healthcare-associated infections
From multidisciplinary communication to establishing safety procedures for construction, remediation and maintenance, facilities teams play a critical hand in reducing patient infections.

Intentional design, seamless care
Thoughtful wayfinding cues and a cohesive aesthetic enable smooth transitions between Endeavor Health Cardiovascular Institute's distinct occupancies.

Working with 'dual-vantage' architects
Certified design expertise aligned with the nuances of health care facilities management bridges the gap between architectural vision and daily operations.