
2026 Hospital Construction Survey results

Image from Getty Images
Hospitals and other health care facilities are fighting increased instances of criminal activity — including cyberattacks. In response, health care officials have increased their physical security and cybersecurity to better protect their staff, patients and visitors.
While these security protections are now being considered at the very start of the planning, design and construction (PDC) process, key stakeholders like security teams and facilities management professionals are not always included in discussions as soon as they should be, according to the new American Society for Health Care Engineering (ASHE)/Health Facilities Management (HFM) magazine 2026 Hospital Construction Survey.
Conducted annually to track budgeting, construction and equipment purchase trends in the health care field, the 2026 Hospital Construction Survey also took a detailed look at the security and cybersecurity considerations of health care facilities — given many physical environment factors can either help or hinder improvements in these areas.
Security challenges
The survey of nearly 300 health care professionals explored the impact of design on creating safe and secure facilities, the involvement of security and facilities personnel in health care facilities planning and design, and the security and cybersecurity challenges that officials prioritize most when designing and renovating facilities.
“Health care workers today are the most likely to be victims of workplace violence; that and cybersecurity issues are driving a lot of changes,” says Michael Lauer, MBA, vice president of emergency preparedness, environmental health and safety, and public safety at BJC Health System in Missouri and chair of the International Association for Healthcare Security and Safety’s Guidelines Council. “It’s critical that security professionals are part of the health care facility planning and design process so that you can embed a multilayered approach to security design. It should start in the parking lot and then have ever-increasing controls as people get into the hospital and closer to the bedside.”
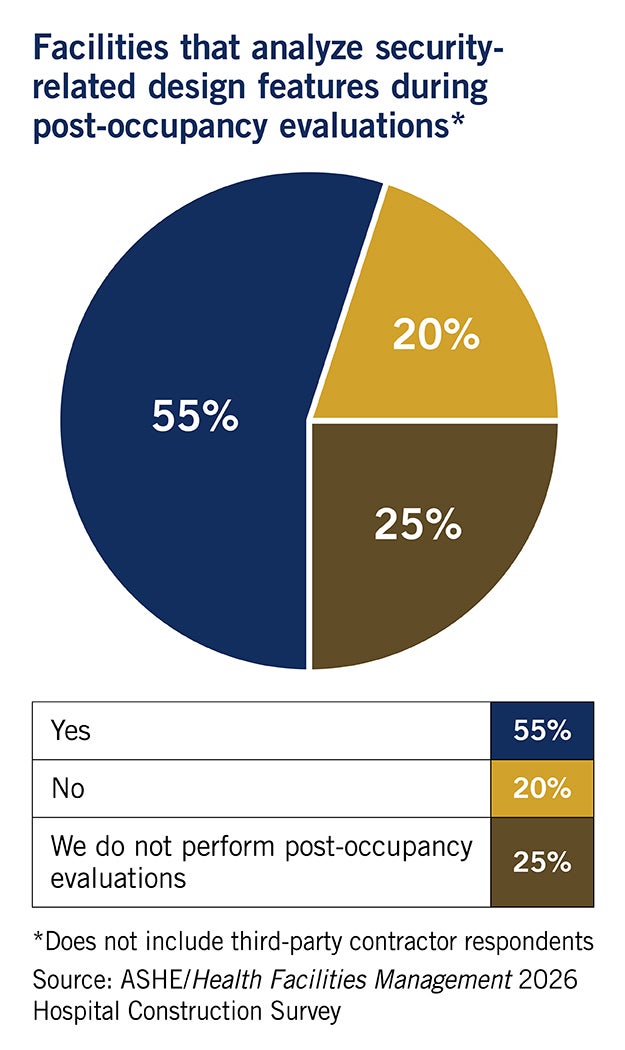
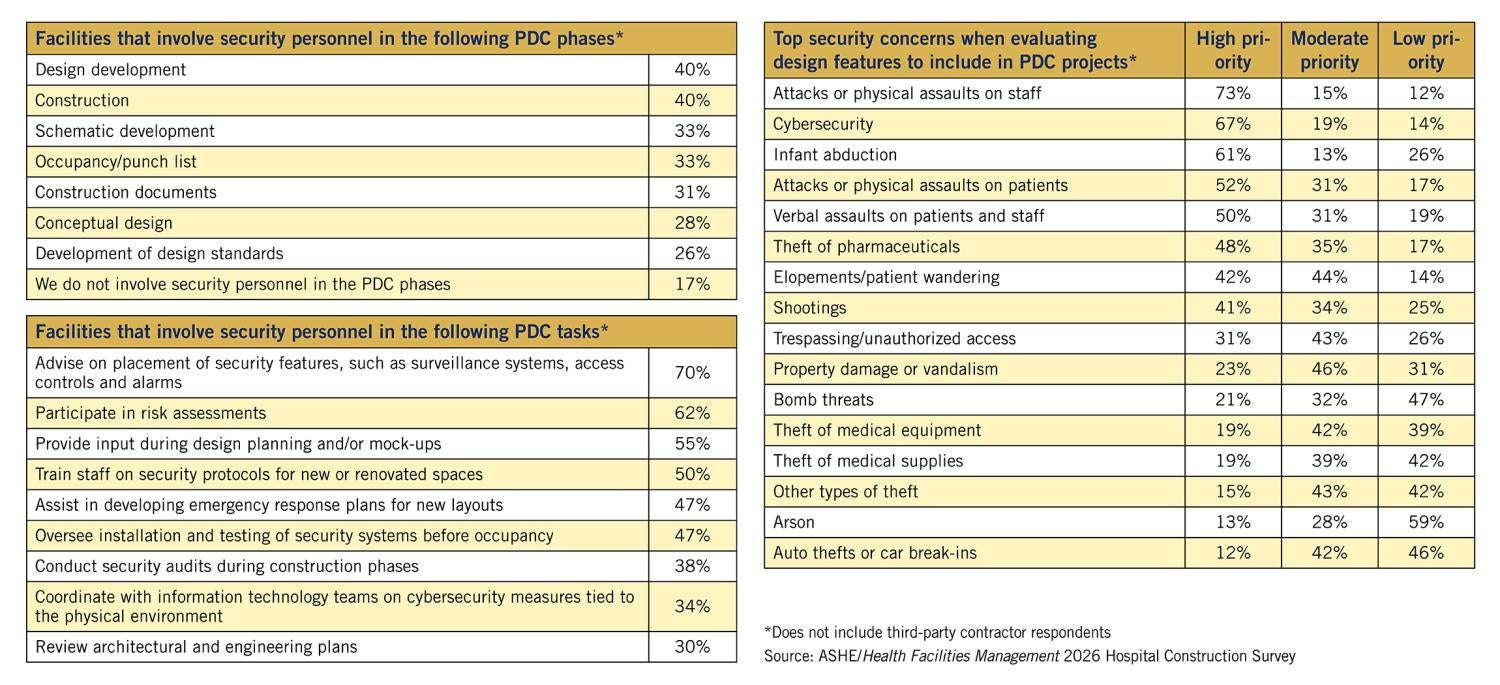
When considering security-related design features in health care construction projects, survey respondents said their highest priorities are adding features that help prevent physical attacks and verbal assaults on staff and patients, cybersecurity, infant abduction and theft of pharmaceuticals. While the majority of survey respondents said security personnel are involved in the later stages of PDC, such as advising on the placement of surveillance systems and alarms (70%), only approximately half (55%) said security provides input during design planning and mock-ups, while just 30% involved security officials in reviewing architectural and engineering plans.
Security personnel need to be involved with the PDC process much earlier, Lauer says, and stay involved from the back end of projects to the front end.
“It is critical that the security perspective be brought into the initial design phases. For example, this allows us to reduce costs by implementing security measures in the initial plans of a construction project, as opposed to retrofitting it into a project,” he says. “It is very expensive to add cameras to a project that has already been completed — where if we are included in those initial phases, we are then running fiber-optic cable through the building during construction.”
Another example is facilities that utilize weapon detection systems. In this instance, facilities need to design their entryways to fit those systems while still maintaining compliance with path of egress requirements — areas that security and facilities officials could weigh in on, says Ted Hood, managing principal and Nashville, Tenn., operations manager at TLC Engineering Solutions. “It dramatically changes your ability to have those systems if you have that discussion at the beginning of a project and not near the end.”

Planning- and design-related security features most often recommended by security officials during planning are inserting cameras and fencing in key external areas, like parking lots; ensuring clear sight lines from main windows across a health care campus; installing bollards to prevent vehicles from driving through entryways; developing secure access control plans to fluidly control the restriction or lockdown of facility areas; and installing weapons control systems, Lauer says.
Bringing security in during the planning and design phase also protects staff through the integration of recommended measures like discreet, windowless, locking safe rooms (especially in emergency departments); ideally placed duress call buttons or wearable call button systems; ballistic-resistant windows on customer exchange areas; and closing off-hours gates on pharmacy spaces.
“The security team may be brought in to talk about door hardware during construction documents development, when they really should be brought in at the very beginning of schematic design to talk about security parameters, barriers, policies and protocols that impact the physical environment, the shapes of spaces and how you can maintain the physical aesthetics alongside a layer of physical security,” Hood says.
Another concerning finding of the survey is that only half of respondents said their security personnel train staff on security protocols for new or renovated spaces, Hood says. “You can have the best physical and technological security design, but if you’re missing solid implementation through training on security protocols and policies with all hospital staff, it’s going to fall apart,” Hood explains. “Equally important to installing duress buttons is teaching staff how to recognize risks and de-escalate a potentially violent situation.”
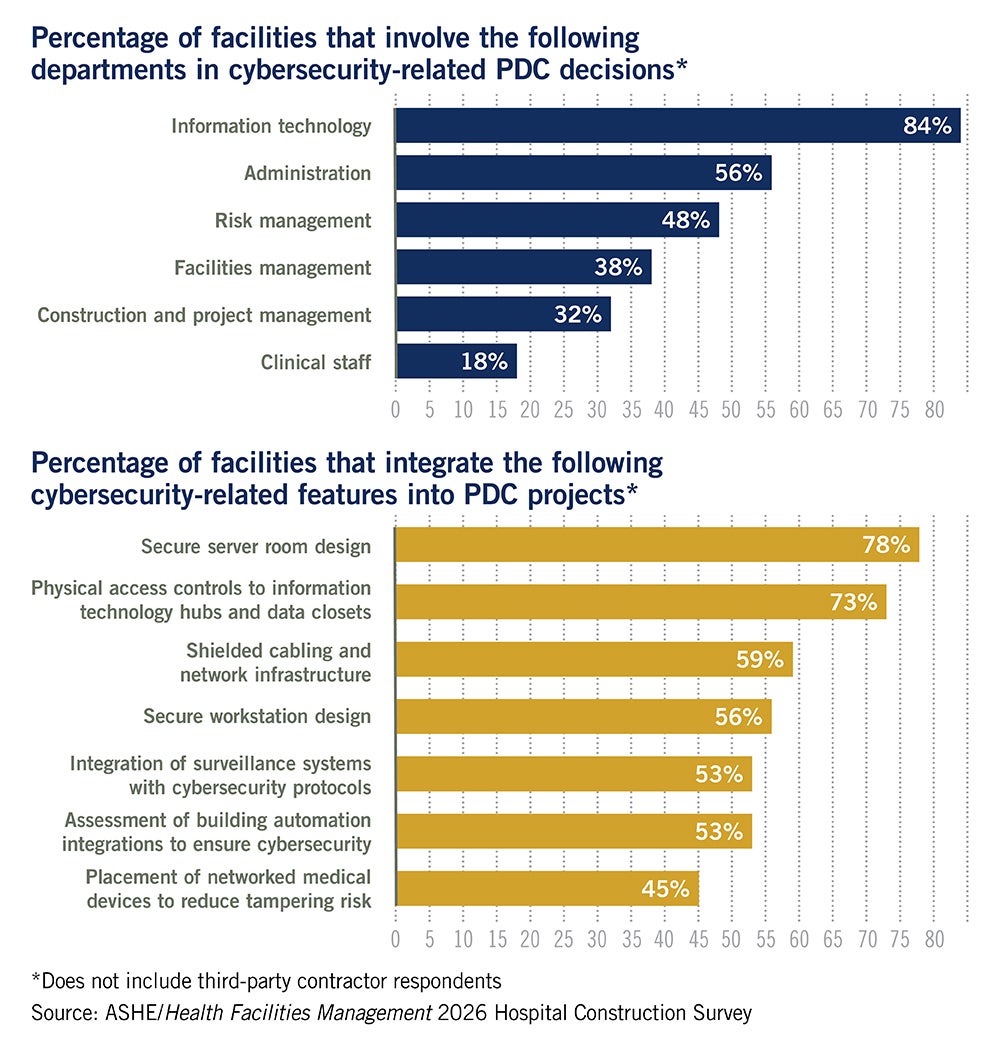
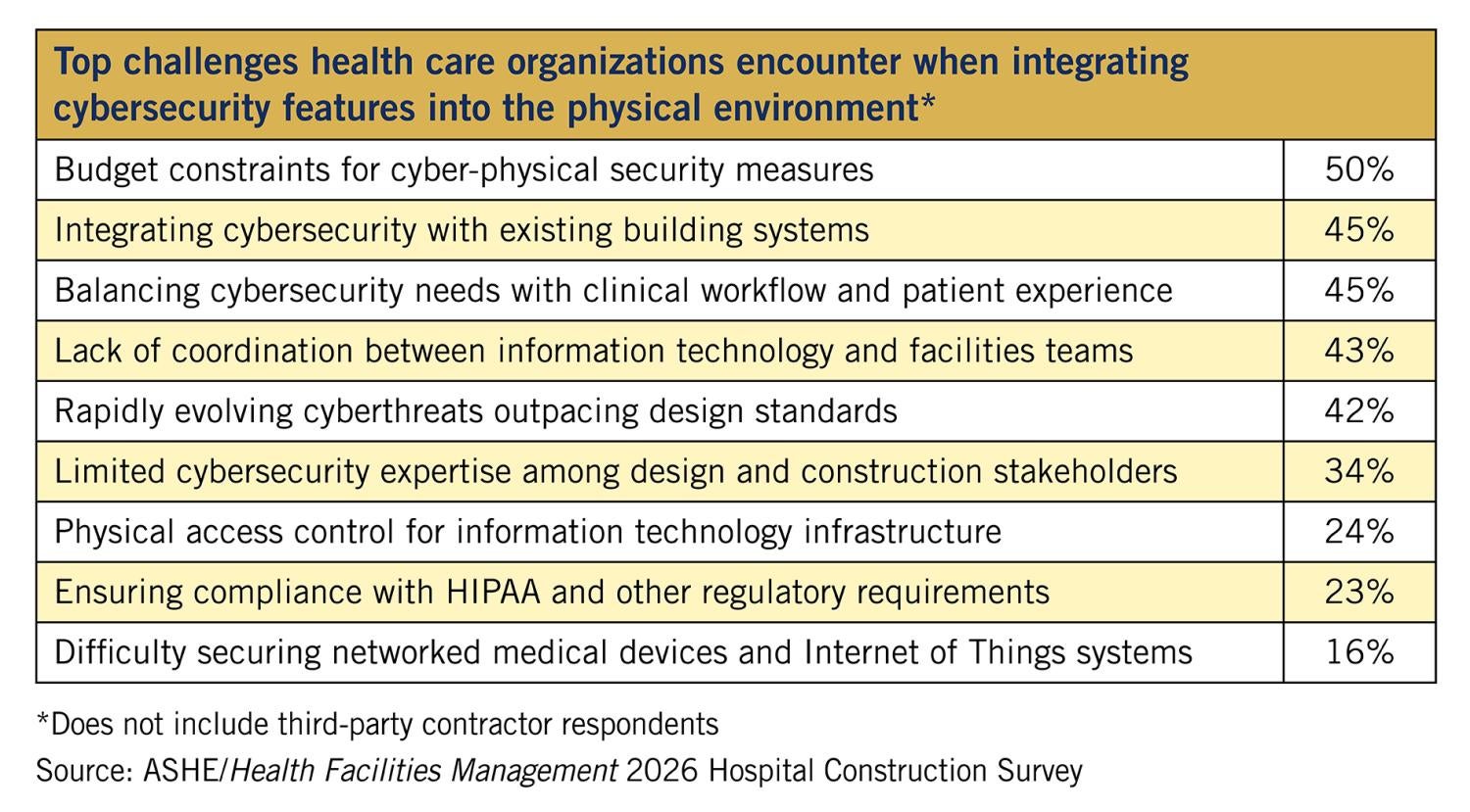
This feedback gap also is prevalent in cybersecurity efforts, with just 34% of respondents saying health care security officials coordinate with information technology (IT) teams on physical environment-related cybersecurity measures. And only 38% said facilities management teams are involved in decisions about cybersecurity-related design features.
“Cybersecurity is something that we frequently see is a complete afterthought on projects,” Hood says. “It then usually becomes an issue once you get into construction and you find there are holes, problems and issues that haven’t been addressed.” One of those issues is not developing comprehensive cybersecurity requirements for all health care facilities and clinical systems, equipment and software — both new and legacy — that connect to the network, especially those developed by third-party vendors, such as building automation systems (BASs) utilizing the network for remote monitoring, that are vulnerable to a cybersecurity attack and put the entire health system at risk.
“The most important thing facilities staff need to realize is that many facilities systems use legacy protocol, they use old technology — and this type of technology can be more vulnerable,” says Jonathan Flannery, MHSA, CHFM, FASHE, FACHE, senior associate director of regulatory affairs at ASHE.
There often are features in BASs; heating, ventilating and air-conditioning (HVAC) systems; and even fire safety systems that connect to a hospital’s network without facilities staff knowing, says Chad Beebe, AIA, CHFM, CFPS, CBO, FASHE, deputy executive director of ASHE.
“Many facilities systems are likely the easiest entry point for a breach in our hospitals,” he says. “Some of those smart features are installed in the background that you don’t know about. [National Fire Protection Association] studies have found that with fire safety systems, there is a lot of built-in connectivity that owners aren’t aware of. It is important to pay attention to security as a whole and be part of that across the organization. Cybersecurity is something that needs to be addressed at a high level, and facilities professionals need to be part of that conversation.”
It is important that security teams are consulted at the start of PDC efforts so they can recommend physical design cybersecurity measures. For example, for years many hospitals had their network servers stored in dual-purpose rooms that also contained supplies or storage, which increased the number of people who could gain access. Best practice now calls for building-dedicated server rooms with strict access controls and camera monitoring to help prevent cybersecurity incidents, Lauer says. “It is critical that we lock down those spaces similar to how we lock down a pharmacy,” he adds.
The challenge to the health care field, Hood says, is to establish security while not making a hospital look like a prison. “It’s an aesthetic challenge that’s been around a very long time, but it is more critical to health systems now than ever before — and I think people are willing to integrate aesthetics and security as part of comprehensive design,” notes Hood.
More on time and on budget
Other survey results looked at what building systems and equipment are most often being implemented and how often PDC budgets and timelines have kept on track. While the effects of the COVID-19 pandemic continue to linger over the health care construction industry in the form of supply chain issues and labor shortages, the ability to deliver projects on time and on budget is continuing to improve.
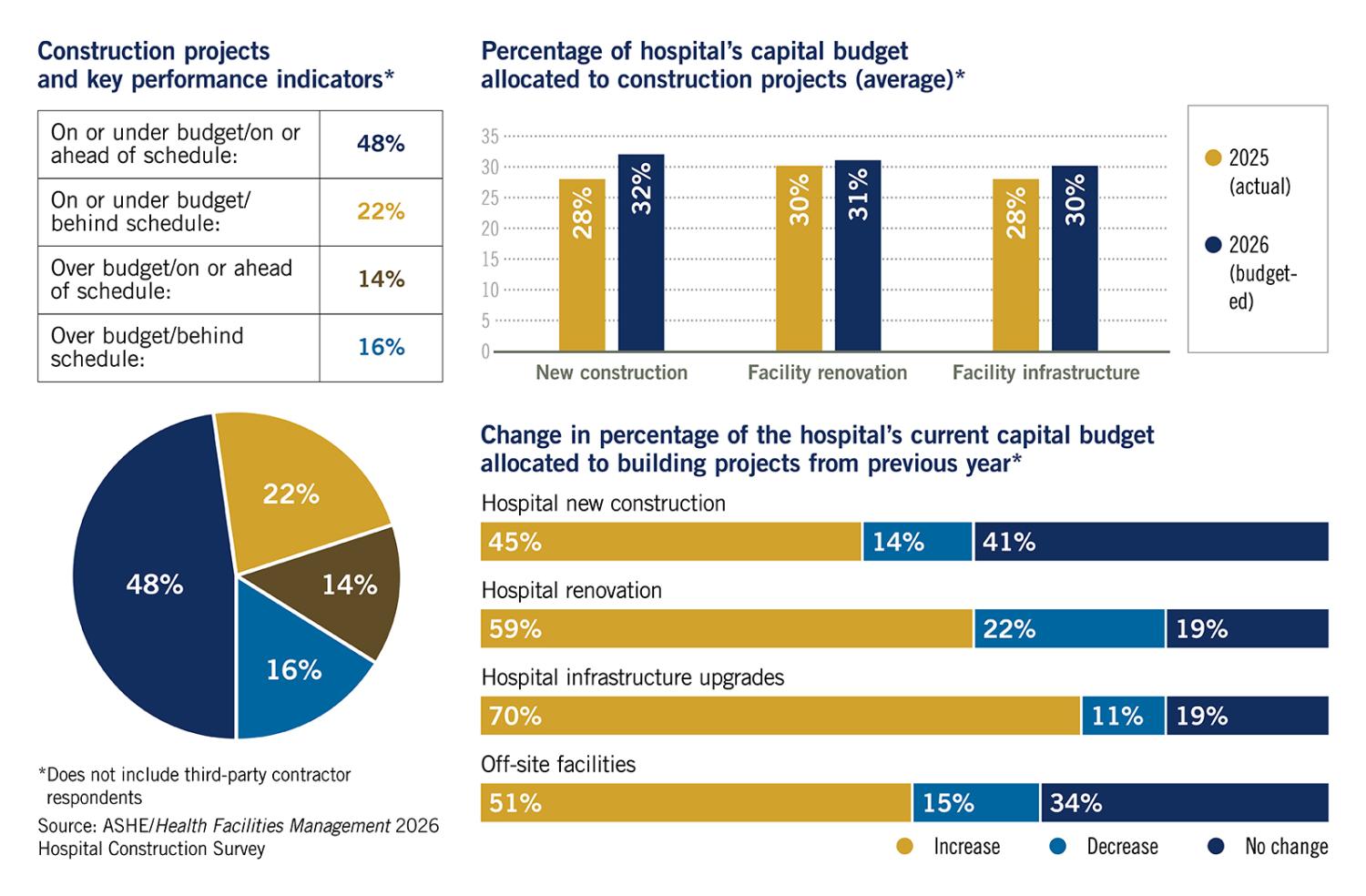
Click chart to expand and view data on construction budgets and key performance indicators
Survey respondents said they were behind schedule and over budget on projects 16% of the time in 2025, a large drop from 2024, when 25% of projects fell into this category. Also, those reporting they are on or under budget and on or ahead of schedule on PDC projects increased from 47% in 2024 to 48% in 2025. While there have been some improvements in the market on inflation and supply chain issues, these budgeting and scheduling improvements are likely due to project teams getting used to and adjusting for the new norm, Beebe says.
“PDC teams have figured out how to manage the labor shortages and supply chain issues since the pandemic threw things out of whack,” Beebe says. “So, ordering escalators two years in advance before they are even inserted into the project design, for example. It comes down to better planning.”
Flannery agrees, saying the field is experiencing the “plateau effect.”
“As we get used to this new norm, we are scheduling better and budgeting better,” he says. “Health care facility project managers are still seeing long lead times, supply chain issues and shortages of labor, but they have become better at planning for these issues.”
While things are improving, they are not yet at pre-pandemic levels — which saw survey respondents reporting that 50% to 60% of their projects were on or under budget and on or ahead of schedule, notes Pete Maslenikov, a health care construction project executive at Skanska USA Building Inc.
Skanska’s own market trends analysis aligns with the survey, though Maslenikov says there are signs that the supply chain is improving and may even get close to pre-pandemic conditions. Labor shortages are expected to continue, however, as other industries, like new data center projects being built around the country, continue to put pressure on the market and take resources away from health care construction projects by paying above-average wages for labor.
Capital budgets up
More funding is available for capital projects this year, according to the survey, with 2% more being budgeted for new construction in 2026. Hospital infrastructure budgets also increased, which may be a result of the pandemic causing many hospital leaders to take a hard look at the role facilities and equipment play in care and the mounting deferred maintenance lists held by many in the field.
“There has been a pretty powerful magnifying glass placed on facilities and their impact on patient care over the last five years, and I believe it has opened the eyes of hospital leaders that we need to take care of our buildings if we want to take care of our patients,” Beebe says. “Your biggest patient is your building, and you have to take care of yourself before you can take care of others.”
An increased need for more acute care patient beds, driven by the aging baby boomer population, also is driving up spending on health care facility expansion construction, Maslenikov says.
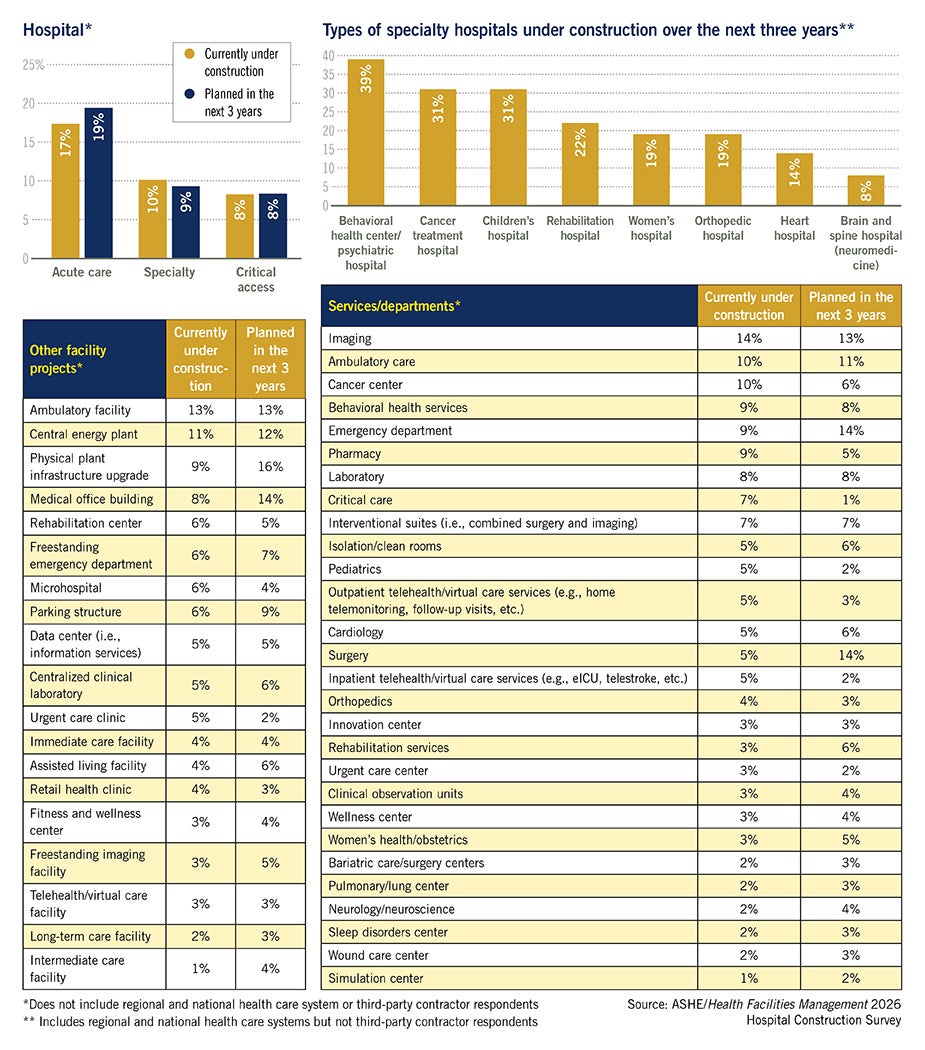
In another trend, hospitals are turning to microhospitals (emergency department-focused small hospitals), which are less expensive to build but maximize community engagement by typically being placed in underserved areas. The 2026 survey found 6% of respondents are currently building a microhospital, with 4% planning one in the next three years — a big jump in a category that is typically less than 1%.
Top building equipment projects
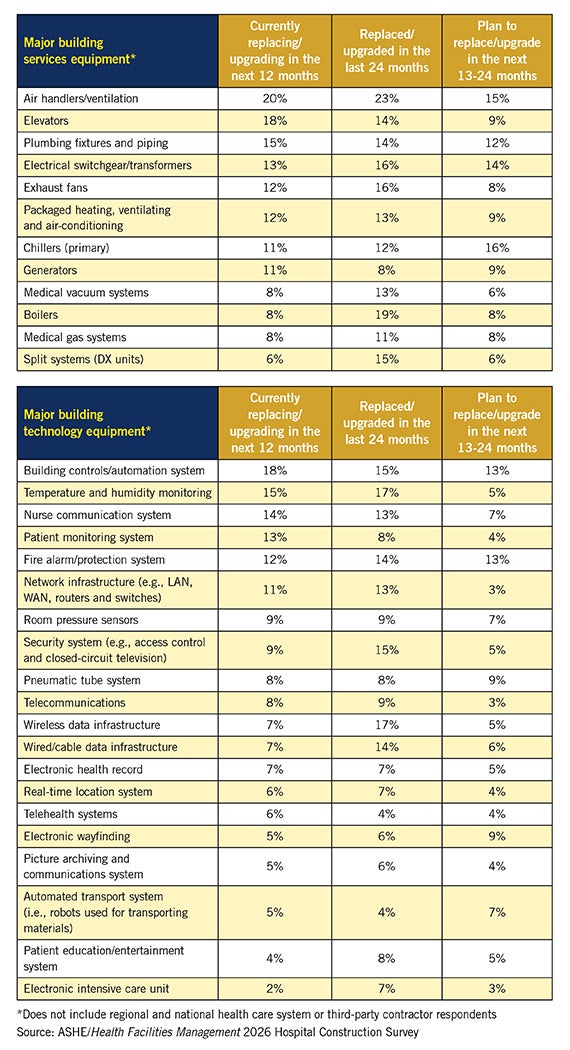
Air handlers remained the No. 1 building equipment project currently being replaced or upgraded over the next 12 months (20%), according to the survey — a position it’s held since 2019. A new addition to the top 5 list of equipment projects this year is packaged HVAC, which 12% said they are installing.
{kind=link}
{kind=link}
{kind=link}
Air handlers took center stage during the pandemic, when hospitals worked to upgrade their HVAC systems in support of better infection control and air filtration. Though officially in the rearview mirror, the pandemic likely is still driving this push to update air handlers and HVAC equipment, Beebe says.
“The way budgeting and financing is structured for capital projects, there is always a long lag between discovery of an issue and getting the funding for improvement,” he says. “We are still in that pandemic bubble, where COVID-19 causes us to sharpen our pencils and ensure we are keeping the facility safe. We might be in that bubble for the next 20 years — something we experienced when sprinklering mandates were enacted.”
The sheer number of air handlers in larger facilities — often totaling 50 or more — also may be a factor in the survey results, Flannery says, as facilities look to get ahead of maintenance costs while also ensuring superior airflow, compliance with ventilation regulations and energy efficiency. “Because you have so many [air handlers], you have to continuously work on them and upgrade them. It is a never-ending project,” he says.
About this survey
SPONSORED BY
Health Facilities Management (HFM) magazine surveyed a random sample of 8,562 hospital and health system executives and third-party architecture, engineering and construction professionals to learn about hospital construction trends. The response rate was 3%.
HFM thanks the sponsors of this survey: Aptitude in Atlanta, and Schneider Electric in Boston. ![]()
On building technology, patient monitoring systems moved into the top 5 for the first time on the survey — with 13% reporting they are replacing/upgrading their system this year, compared to previous surveys where the system hovered in the 5% to 7% range.
One factor driving this increase is likely the current shortage of clinical staff in many hospitals, causing officials to turn to technology to help fill the gap, Maslenikov says.
Recent advancements in these systems, including wireless sensors and wearable tech, artificial intelligence and data processing, and even patient room cameras and video communication systems, also may be driving hospitals to implement the latest and greatest patient-facing systems to meet consumer demand and to stay competitive with other organizations.
Hospitals also are seeing an increase in the acuity of patients, raising the number that need to be on telemetry, Flannery says. This increase, also caused by the aging baby boomer population, likely is leading many facilities to upgrade their patient monitoring systems.
Real-time location systems (RTLSs), which allow the tracking of staff and equipment around a health care system, also saw a jump in implementation in this year’s survey. Technological advancements in RTLSs that allow not just location finding but the tracking of data as well likely are driving increased implementations, Flannery says.
“[RTLSs] greatly increase efficiency,” he explains. “It means I don’t have to get six people out looking for the location of an errant IV pump or fire extinguisher. I also can rely on the system to tell me based on weight if that fire extinguisher is full or needs to be serviced,” he says.
Focus on infrastructure
While the top building project currently under construction remained acute care hospitals (a position held since 2019), central energy plants moved into third for the first time, behind ambulatory care. A total of 23% of respondents said they are building a new central energy plant within the next three years, with 11% having projects currently under construction — up from just 5% to 7% in previous years.
One thing driving this increased demand for power is more hospitals moving toward the electrification of their systems, both to save costs and to reduce their carbon footprint, which in some areas of the country is being required by local regulations.
Projects of this nature take years to plan, meaning many of the central energy plants being built in 2026 were started four years ago — which is when ASHE and others in the field started sounding the alarm on the risks of deferring maintenance and infrastructure upgrades, Flannery says. He expects this trend to continue as more hospitals heed the call to focus on infrastructure enhancements.
“As the survey showed with capital budgets, we are finally getting actual budgets that reflect the change we started calling for four to five years ago,” Flannery says. “People have accepted the reality of it, know they must do something to address it and are now investing in infrastructure.”
Article by Chris Dimick, content development and communications manager at the American Society for Health Care Engineering and production editor at Health Facilities Management (HFM) magazine, and data by Jamie Morgan, senior editor of HFM.
Related Articles

The facilities manager’s role in reducing healthcare-associated infections
From multidisciplinary communication to establishing safety procedures for construction, remediation and maintenance, facilities teams play a critical hand in reducing patient infections.

AdventHealth expands in Tampa Bay with new patient tower
Expected to open in 2029, the new six-story patient tower at AdventHealth Carrollwood will expand inpatient and surgical services for the rapidly growing area.

2026 Vista Award winner Morristown Medical Center
The winning infrastructure project required an untangling of existing systems to provide durable electrical power.