
Making room for building systems

Mechanical rooms and systems that must be planned include chiller rooms, boiler rooms, pump rooms, air movement equipment, cooling towers and similar spaces.
Image courtesy of Stantec
What are “forgotten spaces” in health care design? Simply put, they are spaces no one planned for in the design process — usually mechanical electrical plumbing (MEP), fire protection (FP), information and communication technology (ICT), and core/shell spaces — that are essential requirements in today’s health care facilities.
Forgotten spaces can be costly and time consuming for design and construction teams to resolve, especially when they are discovered late in the process. So, it’s important for project teams to account for them in the initial health care building design.
Why is space forgotten?
Architects and engineers look at the design process differently. Architects see design as the creation of a harmonious whole, section by section. Engineers, on the other hand, tend to view design as the integration of a series of systems.
Each approach has merit, but when pursued separately, it can lead to gaps in design documentation, resulting in forgotten spaces. These apparent gaps can be seen when comparing architectural and engineering drawings.
Architects fill their drawings with detail about the spaces but tend to describe MEP/FP/ICT engineering system spaces sparsely. Conversely, engineers produce drawings that are heavy on detail about headend and distribution spaces for systems.
With the proliferation of building information modeling and other digitally shared drawing tools, this contrast is less apparent. But the printed drawing world is where construction communications reside, and when the documentation is printed, these divergent viewpoints are exposed.
These gaps in architectural and engineering documentation may lead to overlooked details requiring coordination. Occasionally, oversights between the architect and engineering team members result in insufficient space planning that requires design changes of significant magnitude.
This can mean more questions and requests for information during construction — ultimately leading to change orders to resolve uncomplete, uncoordinated or missing content. In extreme instances, entire spaces are forgotten and must be designed into the project later.
But the term “forgotten spaces” also refers to the frequent underestimation by health care space programmers of the amount of space required for engineering systems and core/shell elements.
Early programming
Space programming, when completed during early design phases for MEP, FP and ICT spaces (also known as engineered systems) as well as other core/shell support spaces, is critically important to the success of any project.
Designers are increasingly challenged with identifying best fit solutions earlier in design, often while contractor-led pre-construction efforts around constructability, equipment selection, schedule and cost estimation are being addressed. The importance one places on outlining all engineered and core/shell systems is directly related to overall project budget and schedule integrity, but also to ensuring that rework in space programming, layouts and planning is eliminated.
Architects, engineers and clients can measure the benefits of early space programming in time and money. For example, one should consider the cost that would be required to move an electrical room only 4 feet as the project timeline progresses.
When this move is made during concept and schematic design, the change is simply a matter of adjusting narratives and block diagrams for designers. At design development, however, the cost of relocation becomes significant due to its impact on multiple design trades and pre-construction exercises, such as budgeting and modeling.
During the construction document (CD) phase, the impact of moving a room can multiply fourfold due to the complexity of redesign and tasks borne by the designers and construction trades. An electrical room could be relocated during permitting or construction, but such a design change would be extremely disruptive.
If the cost to move the room during schematic design is $30,000, the cost during the CD phase could easily exceed $250,000 and over $1 million during construction — all to move a room 4 feet. At what point does it become cost prohibitive is a question only the project team and owner can answer.
Real-world examples
Take the coordination of the systems for the 2.1-million-square-foot Feinberg Pavilion and Galter Pavilion at Northwestern Memorial Hospital from 1992 to 1999, and Northwestern’s 1-million-square-foot Prentice Women’s Hospital from 2000 to 2007, in Chicago.
An early analysis of the spatial needs for the connected Feinberg Pavilion and Galter Pavilion drove the programming of Prentice Women’s Hospital’s engineered systems. By reviewing two very large health care projects, one can think about forgotten spaces and how they were prevented on these projects, but also the best practices the team developed for space planning on large health care facilities.
{kind=link}
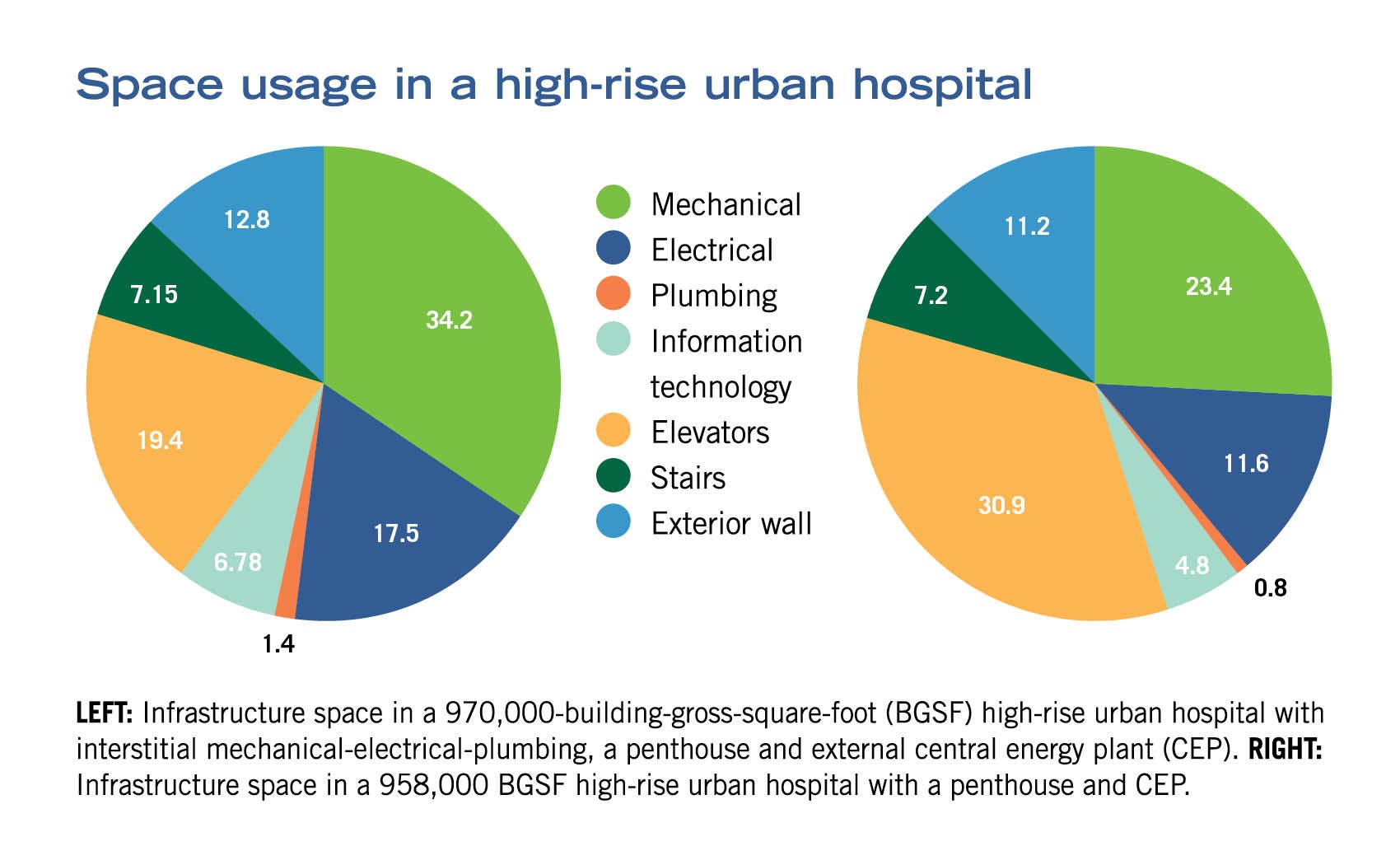
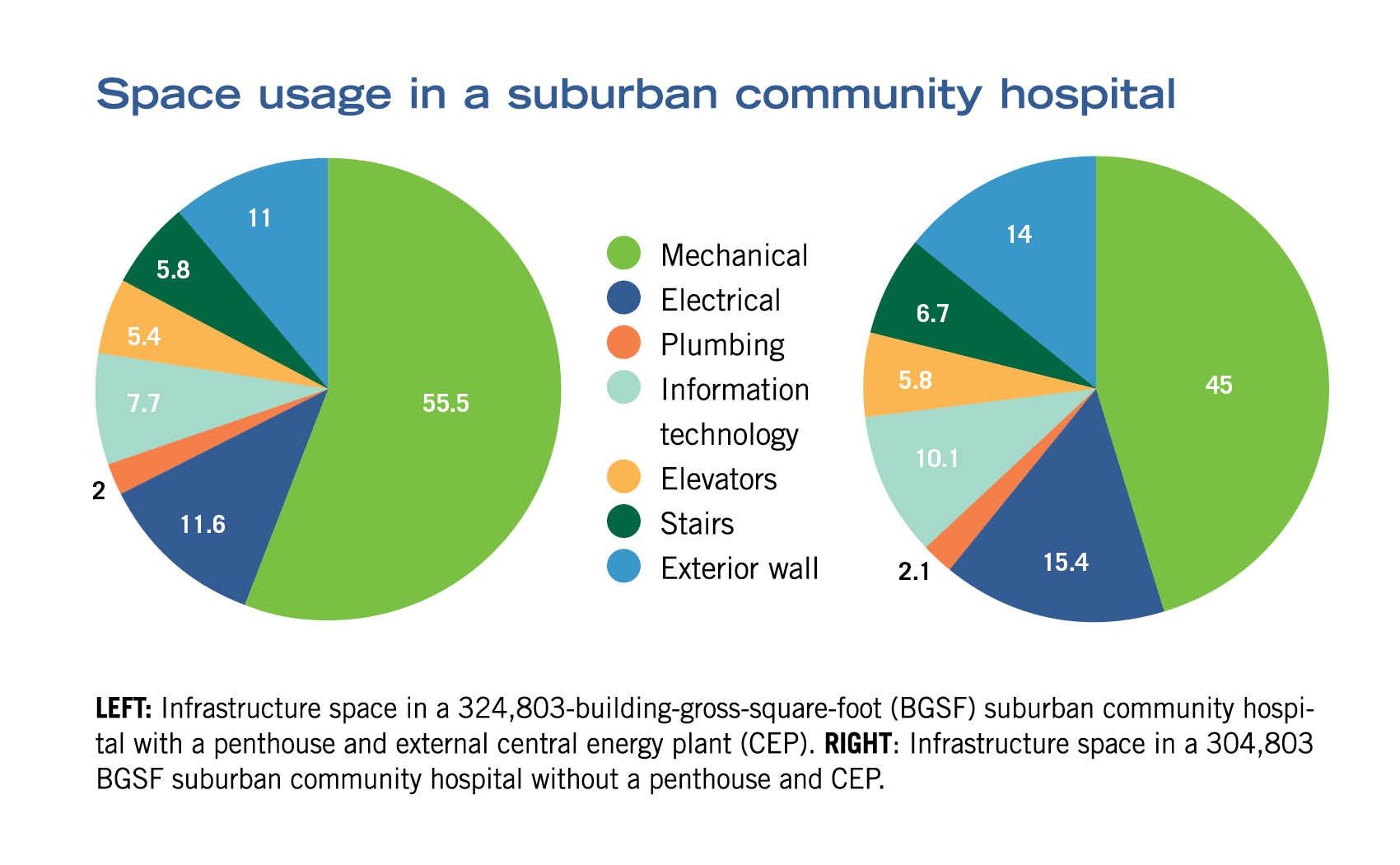
The biggest revelation from the experience with these two projects was the amount of space dedicated to engineered systems and core/shell spatial needs that health care facilities require: 23% to 26% of total space, depending on building configuration. Typically, engineered systems and core/shell elements are the largest space users in a health care facility by far and thus deserve enhanced attention during the design phase.
In benchmarking both urban and suburban hospitals, however, it is notable that departmental space allocations typically seen in space programs do not accurately capture all of the possible engineered and core/shell systems found in hospitals. This discrepancy results in forgotten spaces.
What are these categories of frequently overlooked spaces? Can a categorical list of these spaces promote analysis and inclusion in future health care design space programs? There are eight categories of forgotten spaces typically seen in health care facilities (see sidebar) and a careful analysis of these can, indeed, lead to their inclusion in future projects.
Special requirements
To better understand the special requirements of all the MEP, FP and IT spaces found in a hospital, designers and engineers need to effectively view each as an engineered system.
Viewing these systems as three separate components (main equipment, connector, and signal generator or “collector”) helps them conceptualize the actual systems needs. For example, if a sump pump is main equipment, it will require piping (the connector) and drains (signal generator). When all three of these elements are understood as an engineered system, the different spatial requirements of each become clear.
{kind=link}
Every system has a main equipment, signal generator or collector, and a connector between the two. For example, fire pumps are connected by mains to fire alarm devices; emergency generators are connected by a ductbank to the receptacles; boilers and chillers are connected by piping to coils; air handlers are connected by ductwork to supply and return diffusers; sump pumps are connected by piping to drains; water pumps are connected by piping to incoming water service; and the fire command center is connected by piping to tamper/flow/strobe switch controls.
One of the challenges that designers and engineers face when discussing space is consistent units of measurement. D. Kirk Hamilton and Sarel Lavy discussed this topic in an American College of Healthcare Architects-contributed article in the January 2018 issue of Health Facilities Management magazine that was based on an American Society for Health Care Engineering monograph (see the ASHE Resource box on this page).
Hamilton and Lavy surmised the space requirements for engineering systems and core/shell elements affect space needs at the net square foot (individual room) level, departmental gross square foot (DGSF) level and, most dramatically, at the building gross square foot (BGSF) level.
Misunderstanding the difference between DGSF and BGSF can result in a design that underestimates the space needed for core/shell spaces in a health care facility. This confusion underscores the need for teams to estimate and capture engineered systems and core/shell space requirements in a program early in the design process to achieve a finite understanding of the needs of a project.
One suggestion to avoid underestimating is to create a detailed and accurate space program to reflect accurate figures for each of the eight categories of space that are identified in the sidebar. The rigor of creating this space program will involve exercises for determining individual system needs and requires earlier analysis of engineering systems and core/shell approaches than in traditional programming and planning.
This also requires design teams to engage engineering and technical leadership in the development of the spatial needs. By requiring engineers and architectural technical teams to rigorously justify spatial needs via test fits as the planning team would for a major department, the project team can avoid underestimating space needs in the future.
On any project, designers use the appropriate tools and processes early and often to ensure they define all required spaces. For core/shell and engineering systems spaces, it should be no different. Here are the key tools to consider using:
Develop a program for the engineering system and core/shell space. This can be combined with the project space planning or can run in parallel early in the process to allow for critical focus.
Perform early studies and test fits. Teams can determine the range of space required for the project by optioning studies and floor plans to confirm that requirements can be accommodated within a specific space. The ideas can be put down on paper or in the model. Teams should consider the systems and design concepts that should be evaluated to best determine the design elements that need to be accounted for in the full space program.
Benchmark with past projects and spaces. To gain a fuller perspective on space needs for any project, teams should look at a wider sampling of cases. They should review these cases, and record the different spaces and their total area allocation for reference and guidance. Teams should use the benchmarked data to help address all of the forgotten space.
Capturing needs early
The ability to develop system and equipment concepts early in the design phase and in harmony with the clinical and support space planning can help teams capture space needs early. This can be facilitated by owner and user alignment on the design concept, cost modeling that keeps pace with design concept, material, labor escalation and strong awareness of code requirements.
If the design and owner team can align on details such as facade selection and thickness, structural grid development, lateral system definition, shaft size and placement, equipment selection, stairs and vertical transportation, it will enhance the ability to define space needs upfront.
One might wonder if there are risks to accelerating design decision making and arriving at a completed space program early, say, at the end of schematic design. Certainly, there is risk to accelerating tasks versus following a traditional schedule. A project team must weigh the benefits, risks and costs of embracing an accelerated process as well as the project’s delivery model.
Collaborative delivery models such as design-build, design assist or integrated project delivery (IPD) rather than traditional design-bid-build can help foster better and earlier decision making, better certainty in pricing, and a more streamlined coordination and construction process. Regardless of delivery method, the project team must carefully evaluate all the factors and the associated risks of accelerating.
If design and engineering teams consider the process, mindset and tools discussed previously, they can minimize the occurrence of forgotten spaces. But it’s unlikely they can eliminate them entirely. They need to catch the forgotten spaces as soon as possible in design, and certainly before construction begins. There’s always room to improve, as they must be prepared to contend with forgotten spaces whenever they pop up.
Once discovered, it’s imperative that designers address forgotten spaces with the project team immediately. They can solve the problem together by creating a small task force with representatives from across the team (including construction) to mitigate issues arising from accommodating the space. This task force should work in a “charrette mindset” so that all possible options are quickly and effectively evaluated. They should go back and revise the space program, all while addressing the spatial needs with the owner and construction team.
Time is paramount when designers are developing spatial needs for engineering systems and core/shell spaces. Project delivery methods involving a broader team engagement early in the process (e.g., IPD, design/build, construction manager as agent and construction manager as adviser) work best. Having the key subcontractors for the engineered systems on board would be a bonus toward accurate spatial justification for engineering systems.
However, any approach that engages the engineering team and technical architectural team in determination of accurate spatial needs for engineered systems and core/shell spaces should yield rewards for the project. This engagement can help ensure a project smoothly transitions from early conceptual planning to the detailed design phases and, ultimately, into construction without significant surprises resulting in change orders and their budgetary impacts.
Better-built care
The later forgotten spaces are caught in the process, the more costly and inconvenient they are. There are two major reasons for forgotten spaces in complex health care building projects: lack of coordination between architecture and engineering systems early in the design process, and inaccurate benchmarking of space requirements for health care.
By changing how and when architects and engineers collaborate on design and employing more realistic benchmarking, the possibility of forgotten spaces can be mitigated if not eliminated. If teams engage in project space programming early and use some of the tools described previously, it will result in better allocation of space for frequently forgotten engineered and core/shell spaces and produce a better-built care environment.
About this article
This feature is one of a series of articles published by Health Facilities Management in partnership with the American College of Healthcare Architects.
Douglas J. King, AIA, NCARB, ACHA, is vice president for health care at Project Management Advisors in Chicago, and Jeff Hankin, PE, is senior principal for buildings and health sector engineering lead at Stantec in San Diego. They can be reached at dougk@pmainc.com and jeff.hankin@stantec.com.
Related Articles

Working with 'dual-vantage' architects
Certified design expertise aligned with the nuances of health care facilities management bridges the gap between architectural vision and daily operations.

Advocate announces $1 billion investment in Chicago's South Side
A new $300 million hospital will replace a century-old facility as part of a broader $1 billion investment to expand access, modernize care and address long-standing health issues.

New children's hospital integrates play and movement into care
MultiCare Mary Bridge Children’s Hospital recently welcomed its first patients at its new 250,000-square-foot facility.