
Principles for efficient simulation center layouts
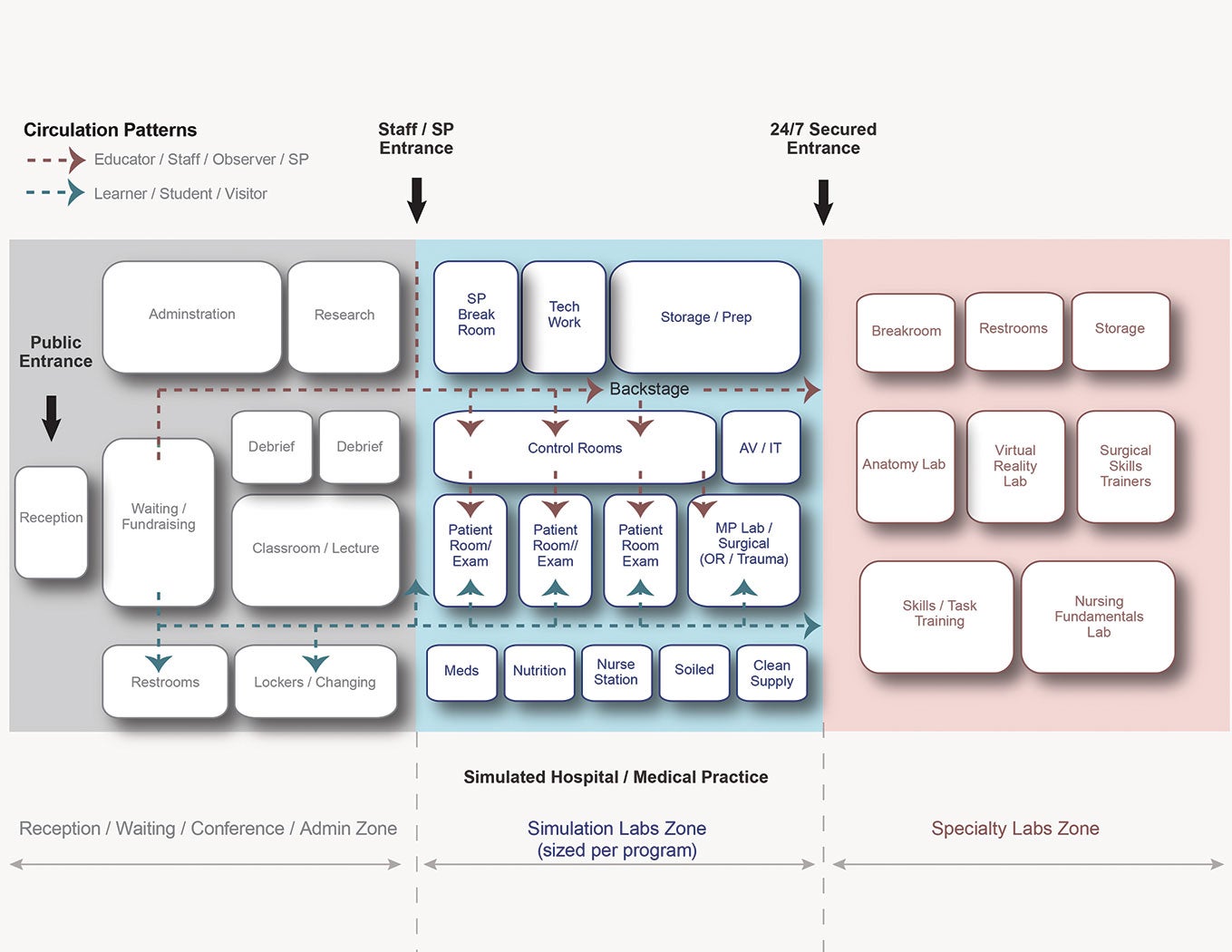
Simulation programs break down into three zones: one for reception, conference/classroom, research and administrative tasks; one for simulated health care labs; and one for labs for specialty skills and task training.
Medical simulation centers are “still a relatively new project type,” says Richard Pizzi, AIA, CEO of Lavallee Brensinger Architects, Boston. There are no official guidelines for the design and construction of this type of program, like those the Facilities Guidelines Institute has written for hospitals and outpatient facilities.
But, in leading the programming and design of more than a dozen medical education and simulation centers in the past decade, including new centers for Yale New Haven Health System and Boston Children’s Hospital, Pizzi has developed some principles for effective and efficient layouts.
According to Pizzi, simulation centers require a space plan layout that considers operations and logistics, critical adjacencies and separate circulation patterns for learners, educators and standardized patients. In general, the program breaks down into three zones: one for reception, conference/classroom, research and administrative tasks; one for simulated health care labs; and one for labs for specialty skills and task training.
In developing the space program for a simulation center, it’s critical to focus on multipurpose spaces. “Every space can and should support simulation,” Pizzi says. A clinical simulation lab can mimic multiple health care settings if it is designed for the space and equipment requirements of each, with walls equipped for multiple headwall scenarios. Labs also can be designed to accommodate in-room debriefing. Specialty skills and task training labs can be outfitted with mobile tables, equipment and infrastructure to support individual training or classroom instruction. Debriefing rooms can simulate consultation, behavioral health and outpatient clinic space. Even support spaces can serve multiple purposes. Kitchenettes can simulate nutrition rooms; storage rooms can simulate clean supply, soiled utility or medication rooms; and single-occupancy toilet rooms can simulate inpatient toilet/shower rooms. Teams can practice patient transport and handoffs in the corridors of a simulation center, and its reception and waiting areas can be used to simulate patient registration, check-in and waiting areas in a clinical setting.
Pizzi stresses that sufficient storage is essential to support such a highly flexible layout.
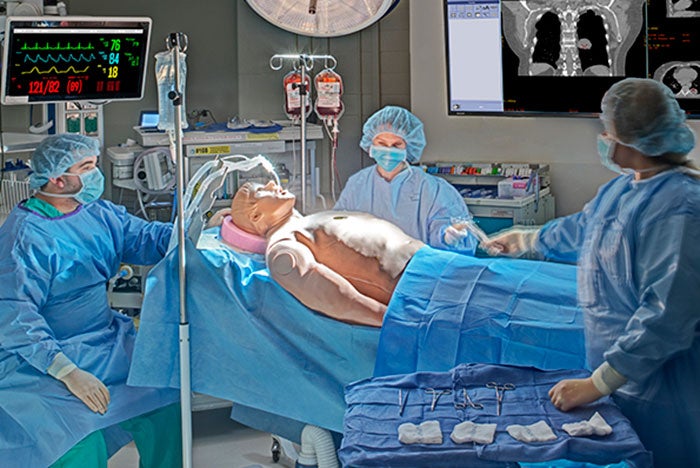
Medical gas supply is among the engineering considerations of simulation center design. The medical gas supply may be a basic system with clean compressed air and vacuum or one that provides oxygen, nitrogen, nitrous oxide and carbon dioxide. Other engineering concerns include the support of simulated normal power loss and the use of emergency power, separate cooling zones for each lab, acoustical separation, an audiovisual equipment room and, if applicable, cadaver storage requirements. The design must accommodate the medical equipment to be used in simulations; the simulation equipment itself, such as wireless technology, mannequins, virtual or augmented reality or 3-D printing technology; and the hardware and software necessary to record and review training scenarios.
Finally, says Pizzi, when it comes to a medical simulation center, “location is everything. Don’t bother building it if it is not easily accessible to the learners.” A successful simulation center must be within walking distance of the medical professionals who will be using it. “Simulation centers are expensive to build and the ROI can be difficult to ascertain,” he says. “Health care professionals are very busy, with demanding schedules. Easy simulation center access is essential to promote high utilization, giving your organization the best opportunity for improved patient outcomes.”
Amy Eagle is a freelance journalist based in Homewood, Ill., who specializes in health care-related topics She is a regular contributor to Health Facilities Management.
Related Articles

Intentional design, seamless care
Thoughtful wayfinding cues and a cohesive aesthetic enable smooth transitions between Endeavor Health Cardiovascular Institute's distinct occupancies.

Working with 'dual-vantage' architects
Certified design expertise aligned with the nuances of health care facilities management bridges the gap between architectural vision and daily operations.

Advocate announces $1 billion investment in Chicago's South Side
A new $300 million hospital will replace a century-old facility as part of a broader $1 billion investment to expand access, modernize care and address long-standing health issues.